Posted: March 2nd, 2017 | Author: DoseSpot | Filed under: In the News, Public Policy | Tags: e-Prescribing, e-Prescribing controlled substances, Electronic Prescription, EPCS, health IT, healthcare IT, Healthcare Software, Maine State Mandate, Minnesota State Mandate, Opioid Epidemic, State e Prescribing Law, State e Prescribing Mandate, State Electronic Prescription Law, State Electronic Prescription Mandate, State Mandates, State Opioid Law | No Comments »
It’s no secret that e-Prescribing has its benefits. Many professionals agree that eRx greatly improves patient safety and reduces overall health care costs by lowering potential medication errors. Additionally, the ability to electronically prescribe controlled substances (also known as EPCS) greatly reduces fraud while preventing patients from being able to “doctor shopâ€, or receive multiple prescriptions for the same drug via different prescribers.
According to Paul Uhrig, Chief Legal Officer for Surescripts, between 3-9% of all opioid abusers use or have used forged prescriptions. With e-Prescribing, the ability to forge prescriptions is completely taken off the table. On top of that, with the addition of Prescription Drug Monitoring Programs (PDMPs) now implemented in all 50 states, prescribers are able to see all pertinent data that has been pulled from the patient’s electronic health record (EHR). This inevitably helps them make more knowledgeable and appropriate choices when prescribing scheduled medications.
With so many known benefits of e-Prescribing, and also because of the nationwide opioid epidemic, many states are getting on board the mandate train, which requires that by law, all prescribers must submit prescriptions electronically. There are currently 3 states which have this e-Prescribing mandate: New York, Maine, and Minnesota and many more that already have legislation in the works for an e-Prescribing mandate.
Taking the First Step: Minnesota Mandate
Minnesota was the first state to create an e-Prescribing mandate, which was intended to push all prescribers to establish and maintain an electronic prescription program that complied with state standards (listed here), effective January 1, 2011. According to the Minnesota Department of Health (MDH), Minnesota measures the status of e-Prescribing in three ways: total transactions, enabled pharmacies, and prescriber utilization. They’ve provided the following chart to demonstrate the increase in e-Prescribing transactions since 2008:

We can see that there was a pretty steep jump in 2011, which is when the mandate went into effect. However, the climb from 2011-2013 was slow yet steady.
Reinforcement of the Mandate, or Lack Thereof
The Minnesota Department of Health reiterates that there is currently no enforcement mechanism for not complying with the state’s e-Prescribing mandate. MDH does stress the benefits of e-Prescribing to providers as well as threaten with the possible implications of non-compliance from a patient/healthcare perspective. When the mandate was first released, it was implied that there would most likely be future establishment of enforcement methods. However, as of today, there is still no means of forcing providers to comply with the mandate.
Because there are no negative repercussions to providers who do not comply, there are many that choose to still utilize paper prescriptions, especially when it comes to sending controlled substances. According to Surescripts, only 3.5% of doctors in Minnesota were using EPCS in 2016. Additionally, the Minnesota Department of Health showed that drug overdose deaths increased 11%, reporting 516 deaths in 2014 to 572 deaths in 2015. These statistics could very well be unrelated to each other, but it still goes to show that that there is work to be done in Minnesota in regards to the opioid epidemic and electronic prescribing.
Some Considerations
Even though there is proof that it has its benefits, the challenges that come with implementing e-Prescribing can’t be ignored. Understandably, and rightfully so, prescribers have long expressed that their main focus is on their patients and they generally don’t enjoy being dictated by the government if it means being intrusive in helping their patients. This is especially true when it involves new systems that require onboarding and training time, but it can also be an even bigger challenge for prescribers to find the funds to support the implementation of an e-Prescribing system.
With these two large considerations in mind, it’s important that future states not only allow healthcare software companies and associated practices ample time to get their e-Prescribing systems up and running, but also offer some form of incentive or enforcement mechanism to keep prescribers in compliance. However, it’s even more important to remind prescribers that the perceived difficulty during the transition time in the beginning is minimal in comparison to how many benefits will transpire in the future. It’s all about taking that first step.
Author: Shannon K.
Sources:Â Minnesota Department of Health; Minnesota Department of Health Fact Sheet; MN e-Prescribing Guidance; Decision Resources Group; USA Today; Managed Care Magazine
About DoseSpot
DoseSpot is a Surescripts certified e-Prescribing platform specifically designed to integrate with electronic health record, electronic dental record, practice management and telehealth software. DoseSpot is certified to e-Prescribe controlled substances and has provided simple, affordable and integratable e-Prescribing solutions to healthcare IT companies since 2009. For more information, please visit www.DoseSpot.com.
Posted: February 15th, 2017 | Author: DoseSpot | Filed under: Controlled Substances, In the News | Tags: Addiction Treatment, Alternative Treatments, Care Coordination, Chronic Pain, Chronic Pain Patients, Controlled Substances, e-Prescribing, e-Prescribing controlled substances, EPCS, MAT, Medication Assisted Treatment, Opioid Addiction, Opioid Crisis, Opioid Epidemic, State Mandates | No Comments »
It’s estimated that 100 million Americans struggle with chronic pain, yet most are facing a barrage of obstacles while seeking treatment in order to appropriately manage their pain. With the current opioid epidemic sweeping the nation, people want the number of opioid overdoses to fall, but patients don’t want to be made to suffer, and rightfully so.
Has the opioid crisis and its implications prevented legitimate chronic pain sufferers from receiving the treatment and associated services they require to productively function in life?
As of recently, more than half of prescribers across America are cutting back on opioid prescriptions, and nearly 1 in 10 have stopped prescribing them altogether. They’re ultimately struggling to find a balance about the merits of using opioids to treat pain, especially in the absence of effective and affordable alternatives.
With this reality, it appears that the chronic pain population is facing an uphill battle, especially with the justified fear of prescribers pulling back in such a chaotic way that could be harmful to patients. Opioid drugs affect the body in an extreme manner and are not something a patient should stop abruptly or without appropriate medical oversight. It needs to be a monitored process, especially for those who have been on long term treatment.
In fairness to the other component of the chronic pain equation, are those patients that truly suffer from opioid addiction. As noted in a recent Boston Globe article, physicians face myriad pressure as they struggle to treat addiction and chronic pain, two conditions in which most physicians receive little training and often intertwine with one another.
Addiction is a complex disease that requires multifaceted solutions and a team approach. No single physician can provide the breadth of treatment required, nor are the necessary payment mechanisms in place to facilitate the “entirety†approach to treating addiction. That and the lack of physician education in addiction further fuels the long battle chronic pain patients are currently experiencing. Without proper knowledge of the physician, is every chronic pain patient now being viewed as an addict? Is that a realistic prejudice they’re being faced with?
In many cases, physicians are walking away completely – they don’t even want to see patients in chronic pain, but others urge to partner with patients and stay with them to help find other options. Such alternatives include The Spaulding Program, a program aimed at developing and teaching coping mechanisms, strategies, and “tricks†to manage and get through the pain. Although the program experiences great success, it had to limit its operation 20 years ago due to insurers ceasing payment for their comprehensive form of care.
It’s hopeful that the concern over opioids will lead to improved care, by deepening the doctor-patient relationship and opening the door for conversation to talk about managing pain, thus pointing to the desperate need for alternative treatments. For now, what is a chronic pain sufferer to do?
Author: Mark H.
Sources:Â Health.com; The Hill; American Academy of Pain Medicine; Boston Globe; Kevin MD Blog; CBS Los Angeles
About DoseSpot
DoseSpot is a Surescripts certified e-Prescribing platform specifically designed to integrate with electronic health record, electronic dental record, practice management and telehealth software. DoseSpot is certified to e-Prescribe controlled substances and has provided simple, affordable and integratable e-Prescribing solutions to healthcare IT companies since 2009. For more information, please visit www.DoseSpot.com.
Posted: February 6th, 2017 | Author: Jodi | Filed under: Basics, Dental | Tags: ADSO, American Dental Association, Association of Dental Support Organizations, Care Coordination, Controlled Substances, Dental, Dental e-Prescribing, Dental Group Practice, Dental Industry, dental practice management, Dental Support Organizations, DSO, DSOs, electronic prescribing, EPCS, health IT, Healthcare Delivery Model, Healthcare Software, healthIT, Opioid Epidemic, Oral Health, Patient Engagement, Practice Management Software, State Mandates, Value Based Care | No Comments »
The significant role of oral health and its contribution to an individual’s well-being has come under scrutiny as of late. In 2014, it was estimated that more than 181 million Americans would not visit a dentist because of several barriers to care, or a self-diagnosis of “my mouth is healthy – I do not need to visit the dentist.†Other reasons noted by individuals not seeing their dentist on a consistent basis were: cost or no insurance, limited dental access in their area or lack of transportation, or they simply did not have the time.
With this data in tow, a more efficient and readily available business model has become increasingly popular within dentistry: Dental Support Organizations.
What is a DSO?
According to the Association of Dental Support Organizations (ADSO), Dental Support Organizations (DSOs) contract with dental practices to provide critical business management and support, including non-clinical operations, and range from small to large size organizations serving dental practices throughout the country.
The business models of DSOs do differ and while the neighborhood family dentist typically treats the general patient population, dental practices supported by DSOs often focus on specific populations. For example, some DSOs are entirely focused on meeting the needs of pediatric patients, while others are focused on more rural populations. This is not to say that DSOs do not serve the general population, as many still do.
The Patient Experience
The true patient benefit of a DSO model lies in the integrated technologies and streamlined processes. DSOs offer patients many time saving benefits including:
- Online appointment booking systems
- Online bill pay
- Flat rate appointments
- Flexibility to visit dentists between multiple offices
- Electronic prescription routing

Dental Infographic by Dental Care Alliance
The Role of Technology Within DSOs
DSOs are at the forefront of technology, both from a clinical and administrative standpoint. They pride themselves on remaining innovative, not only to better treat their patients, but to also have a competitive advantage and to attract and maintain new dentists. From billing software to detailed patient charting to specific treatment mechanisms, technology is embedded in nearly every workflow.
While many DSOs have thrown out their dentists’ paper prescription pads and have adopted electronic prescribing (e-Prescribing) software, there is still plenty of room to grow. e-Prescribing software provides dentists with the ability to send non-controlled and controlled prescriptions electronically directly to the patient’s pharmacy which adds convenience to the patient’s experience.
In addition to the prescription writing feature, e-Prescribing includes high value functionality for the dentist, patient and management teams such as:
- Insight into a patient’s current medication regimen.
- Ability to check for drug-to-drug and drug-to-allergy interactions at the point of care to help improve treatment decisions.
- Reporting capabilities that share what is prescribed and in what quantities to assess for in regards to compliance. This is especially crucial with the current opioid epidemic and having the ability to track prescriptions for controlled substances.
- Documentation for both the dentist and the patient including dental specific dosing information, as well as medication monographs.
What’s Ahead for DSOs
DSOs are continuing to shake up the dental industry. New DSOs continue to emerge, while existing ones are frequently acquiring new dental practices, therefore expanding and continuing to growing throughout the country. As previously discussed, cost and limited access to care were the most popular barriers, but DSOs offer streamlined solutions for both barriers as they are committed to the improvement of oral health in the United States through the accessibility of high-quality dental care. It is only a matter of time before more and more dentists hop on board.
Sources: American Dental Association; Association of Dental Support Organizations (ADSO); ADSO Whitepaper; National Institute of Dental and Craniofacial Research; Centers for Disease Control and Prevention; Dental Care Alliance
About DoseSpot
DoseSpot is a Surescripts certified e-Prescribing platform specifically designed to integrate with electronic health record, electronic dental record, practice management and telehealth software. DoseSpot is certified to e-Prescribe controlled substances and has provided simple, affordable and integratable e-Prescribing solutions to healthcare IT companies since 2009. For more information, please visit www.DoseSpot.com.
Posted: January 30th, 2017 | Author: DoseSpot | Filed under: Basics, Public Policy | Tags: e-Prescribing, e-Prescribing Platform, e-Prescribing Registration, e-Prescribing Software, e-Prescribing Solution, e-Prescribing State Mandates, New York e-Prescribing Mandate, New York e-Prescribing Registration, New York e-Prescribing Renewal, New York e-Prescribing Vendor Registration, New York e-Prescribing Vendor Renewal, New York Mandate, New York State Dental Association, New York State Department of Health, New York State Mandate, Registration for Official Prescriptions and e-Prescribing Systems, ROPES, State Mandates | No Comments »

If you are a prescriber in the state of New York, you probably know by now that electronic prescribing (e-Prescribing) of both controlled and non-controlled substances has been mandatory since March 27, 2016. As part of this mandate, all prescribers who will be sending controlled substances are required to register their e-Prescribing software as well as report to the controlled drug registry each time a controlled medication is prescribed or dispensed. In order for users to access the registry, the prescriber must first create an online Health Commerce System (HCS) account. Once the HCS account is active, the prescriber can then access ROPES to register their certified electronic prescribing software application for controlled substances.
The good news is that applying for an HCS account is as easy as filling out an online form and having a New York State driver’s license (or photo ID).
Applying for an HCS Account
Requirements: New York state valid driver’s license or photo ID and New York State Education Department registered medical professional license
To apply, you will need to access the following page: https://apps.health.ny.gov/pub/top.html
After you have applied and have been granted an HCS account, you will be able to sign back in via this link: https://commerce.health.state.ny.us
You may also use the following link as a reference to see in full detail a direct guide of the application process: https://apps.health.ny.gov/pub/ctrldocs/paperless_docp.pdf
In addition to requiring an account in the Health Commerce System (HCS), if prescribers intend to order controlled substances electronically, they will also need to register their certified electronic prescribing application software with the New York State Department of Health, Bureau of Narcotic Enforcement (BNE). This is done by filling out a ROPES form online through an HCS account.
What is a ROPES form?
A ROPES form is a new online application that allows the practitioner/organization to renew their registration for the Official Prescription Program and register their certified electronic prescribing software application for controlled substances. ROPES stands for Registration for Official Prescriptions and E-prescribing Systems. Only the prescriber can access the ROPES application.
Pre-requisite Requirements for ROPES
- Prescriber must be already registered with the Official Prescription Program (OPP)
- Prescriber must have an active DEA registration
- Prescriber must have an active NY license
- Prescriber must NOT be a registered Physician Assistant (PA) – PA’s must continue to submit the OPP registration form (DOH-4329) along with the PA Authorization Form (DOH-5054) to renew their OPP registration.
Completing the ROPES Form
In order for a prescriber to fill out a ROPES form, he/she must log into his/her HCS account (outlined above) by accessing the following weblink: https://commerce.health.state.ny.us and following the next few steps:
- Select “my content†at the top of the page
- Scroll down and select “All applicationsâ€
- Scroll over and select “Râ€
- Scroll down and select “ROPES†and complete the form
The ROPES form requires that the prescriber identifies the third party audit certifying organization and the date of the third party audit. Keep in mind that it is the software vendor that must be certified not the prescriber. The software vendor will supply all necessary information about this certification to the prescriber. The ROPES form must be renewed every two (2) years in order to remain valid. The prescriber must renew their OPP registration first via the one step process prior to renewing their current ROPES registration.
Questions?
Any questions regarding the ROPES form or the process can be directed to the BNE at narcotic@health.state.ny.us or by calling 1-866-811-7957.
For prescribers utilizing DoseSpot who have questions regarding the ROPES required third party audit information, please contact DoseSpot support at 888-847-6814.
Author: Shannon K.
Sources: Practice Fusion; New York State Dental Association; New York State Department of Health
About DoseSpot
DoseSpot is a Surescripts certified e-Prescribing platform specifically designed to integrate with electronic health record, electronic dental record, practice management and telehealth software. DoseSpot is certified to e-Prescribe controlled substances and has provided simple, affordable and integratable e-Prescribing solutions to healthcare IT companies since 2009. For more information, please visit www.DoseSpot.com.
Posted: January 23rd, 2017 | Author: DoseSpot | Filed under: Basics, Controlled Substances | Tags: CMS, Controlled Substances, DEA, e-Prescribing, e-Prescribing controlled substances, e-Prescribing Integration, EPCS, health IT, healthcare IT, Maine State Mandate, meaningful use, Opioid Epidemic, State Mandates, surescripts | No Comments »

Navigating the waters of e-Prescribing can seem like a very daunting task considering the various state and federal regulations. To assist you in understanding, let’s review the information relative to e-Prescribing of Controlled Substances (EPCS) in all 50 states and how your state is measuring up.
Until recently, one-half of all U.S. States prohibited e-Prescribing of controlled substances. The thought was that paper prescriptions were safer and more secure. On September 15, 2015, however, Vermont became the last state to allow electronic prescribing of controlled substances, or Schedule II-V medications, making this process legal in all 50 U.S. states.
“We certainly believe that because of the enhanced security associated with e-Prescribing of controlled substances, the opportunity for abuse, misuse, and fraudulent activity is going to be dramatically reduced,” said Ken Whittemore, BSPharm, MBA, Senior Vice President of Professional and Regulatory Affairs at Surescriptsâ„¢, a nationwide health information network.
With this process now legal in all 50 states, and the safer option at that, it may be surprising to find that as of the most recent data available, only 7% of prescribers are sending controlled substances on the Surescripts network.
So, why the discrepancy? Are pharmacies not accepting electronic prescriptions? Are prescribers not able, or willing, to send these prescriptions electronically? Is this process too difficult? Why is this process used in some states so heavily, but so infrequently in others?
Pharmacies are ready!
In 2010, the DEA published a final ruling giving not only practitioners the option to write controlled substances electronically, but also for pharmacies to receive, dispense, and archive electronic prescriptions.
“It became incumbent upon a number of stakeholder groups in the pharmacy industry to tackle the issue and bring states into alignment with the DEA’s rule,” Ken Whittemore, BSPharm, MBA told Pharmacy Today.
Many pharmacy stakeholder groups, including APhA, the National Alliance of State Pharmacy Associations (NASPA), the National Association of Chain Drug Stores, and Surescripts, worked together over a 5-year period to rework some state laws, a process that can take a long time. Between 2010 and 2015, the pharmacy end of the spectrum worked hard on adoption and enablement, while prescriber enablement trailed. Using data from Surescripts, a study published in the January 2015 American Journal of Managed Care found that pharmacies with technology in place to accept e-Prescriptions for controlled substances increased from 13% in 2012 to 30% in 2013. By contrast, only 1% of all prescribers were capable of e-Prescribing controlled substances in 2013.
However, between 2012 and 2013, the number of e-Prescriptions for controlled substances grew dramatically from 1,535 to 52,423. Talk about a rapid jump!
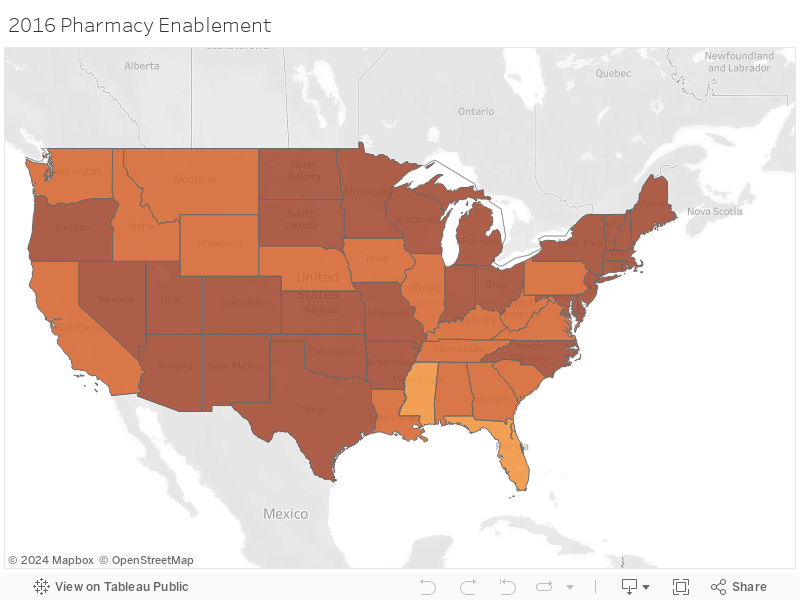
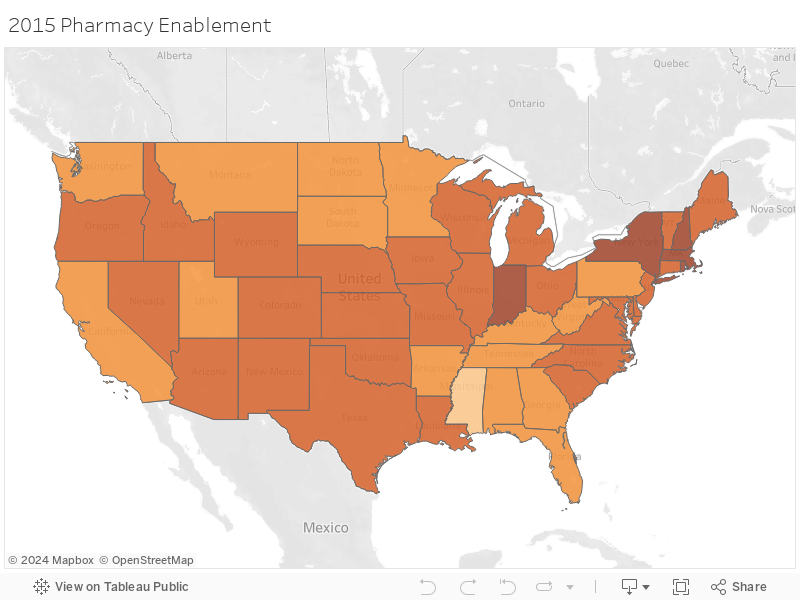
According to the 2015Â Surescripts National Progress Report, an average of 81% of pharmacies were enabled for EPCS in 2015. States including Hawaii and Mississippi were at the bottom of this list with less than 70% of pharmacies enabled, while states in the Northeast such as Massachusetts, New York, New Hampshire, and Rhode Island led this list with over 90% of pharmacies enabled for EPCS.
As of December 1, 2016, these numbers have only risen, with both Hawaii and Mississippi now having over 75% of pharmacies enabled. New York and Maine lead the race on that front with 96.8% and 95.2% of pharmacies enabled currently. This is in large part due to the state mandates put into place in 2016 and 2017, respectfully.
How about the prescribers?
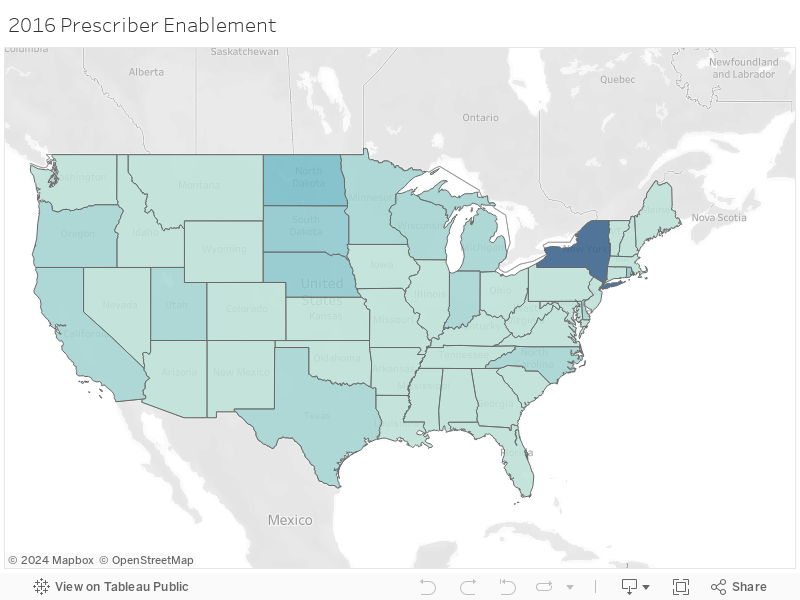
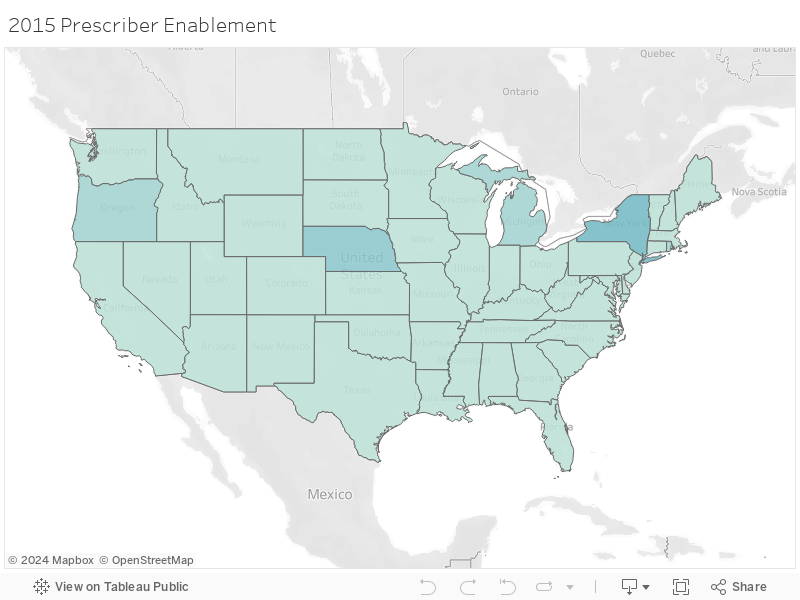
With so many pharmacies enabled for EPCS, and legislature allowing this process in all 50 states, it may be surprising to know that an average of 3.39% of prescribers were enabled to e-Prescribe controlled substances according to the 2015 Surescripts National Progress Report.
Lengthy and time-consuming software auditing and prescriber identity proofing processes are likely factors that have stalled prescriber adoption of EPCS, but for pharmacists, the initial setup is much easier. In addition, there have not been enough incentive for prescribers to adopt EPCS.
e-Prescribing was a requirement under the federal Meaningful Use Electronic Health Record (EHR) program, which incentivizes the use of EHRs through financial payments. However, e-Prescribing of controlled substances was specifically exempted from Meaningful Use Stages 1, 2, and 3. For these reasons, it isn’t surprising that in 2015 the state with the highest number of prescribers enabled was New York, as that was one of the only states with an e-Prescribing state mandate in effect at that time.
In 2015, New York had 26.6% of their prescribers enabled for EPCS, with Nebraska not far behind at 15%. Fast forward to December 1, 2016 and prescriber enablement has grown tremendously in some states, but remain dismally low in others. New York now has 71.5% of prescribers enabled, with no other state having even one-third of their prescribers enabled for EPCS. In fact, the average percentage for EPCS enabled prescribers remains even as of December 1, 2016, at only 8.4% despite all of the benefits of EPCS.
Why are these numbers so varied?
Electronic prescribing of controlled substances (EPCS) reduces fraud and keeps patients from getting multiple prescriptions for the same drug, so why are some states seeing major buy-in while other states are lagging? Much of this is impacted by states that have legislation in place to either require or reinforce the use of e-Prescribing, as outlined below.
Minnesota
Minnesota was the first state to implement an e-Prescribing mandate in 2008 in order to improve quality outcomes and efficiency in health care. The state mandate required prescribers, pharmacists, pharmacies, and pharmacy benefit managers (PBMs) to be up and running with e-Prescribing by January 1, 2011, however, only 13% of prescribers are actually enabled for EPCS as of late. Could this be because legislation doesn’t enforce its own law or penalize prescribers for not adhering to this legislature? Marty LaVenture, director of the Minnesota Office of Health IT and e-Health, seems to agree and notes, “policy levers could be used to encourage full adoption and use of e-Prescribing capabilities.”
New York
As you may already know, New York was the first state to require e-Prescribing of all prescriptions, both controlled and non-controlled, and the first to implement penalties for failing to adhere to this ruling. Penalties include, but are not limited to, loss of license, civil penalties, and/or criminal charges. With the highest rate of prescriber EPCS enablement, it’s evident that New York prescribers are taking this quite seriously.
Maine
Maine is the next state to implement an e-Prescribing regulation as of July 1, 2017 where all opioids prescriptions must be sent electronically. With only 0.6% of prescribers enabled for EPCS in the state according to the Surescripts report, and up to 2.9% as of the beginning of December 2016, it’s clear that Maine has a long way to go for all prescribers to be ready to follow this regulation.
In Summary
Although it’s legal in all 50 states, and there are many reasons EPCS is safer than on paper or another method, there is still a great discrepancy between EPCS enabled pharmacies and EPCS enabled prescribers due in part to the strict requirements put in place on the prescribers. While the statistics referenced here show that provider adoption of EPCS is still low in comparison to the pharmacy adoption we have seen, it’s important to remember that the e-Prescribing of non-controlled substances also took years to reach the level we now see today. It seems the only tried and true way for these numbers to rise quickly and meet the numbers we currently see for pharmacy enablement is to implement regulations and penalties for not adhering to this requirement as outlined in the above state mandates. All eyes are now on Maine to see how their journey goes.
Check out the maps below to see how your state measures up!
Author: Lindsey W.
Sources: American Pharmacists Association; USA Today; Surescripts 2015 National Progress Report; Surescripts EPCS; Minnesota Department of Health; Maine Medical Association; e-Prescribing Blog; CMS
About DoseSpot
DoseSpot is a Surescripts certified e-Prescribing platform specifically designed to integrate with electronic health record, electronic dental record, practice management, and telehealth software. DoseSpot is certified to e-Prescribe controlled substances and has provided simple, affordable and integratable e-Prescribing to more than 150 health care software companies since 2009. For more information, please visit www.DoseSpot.com.
Posted: November 28th, 2016 | Author: DoseSpot | Filed under: Controlled Substances, In the News, Public Policy | Tags: Controlled Substances, DEA, Dental e-Prescribing, e-Prescribing controlled substances, e-Prescribing Integration, e-Prescribing Maine Mandate, EPCS, Healthcare Software, Maine Controlled Substance Act, Maine Controlled Substance Prescription Requirements, Maine Dose of Reality, Maine e-Prescribing Law, Maine e-Prescribing Legislation, Maine e-Prescribing Mandate, Maine e-Prescribing of Controlled Substances, Maine EPCS, Maine Opioid Law, Maine State Mandate, Mandatory e-Prescribing, Mandatory Electronic Prescribing, Opioid Epidemic, Opioids, Prescription Monitoring Program, State Mandates | No Comments »
Maine is well known for its rocky coastline, iconic lighthouses, sandy beaches, and lobster shacks. However, past the classic scenery is where you’ll find the state dealing with a crisis that others across the United States are also experiencing: the opioid epidemic.
In 2015, Maine suffered an astounding 272 drug overdose deaths, following 208 deaths of the same cause in 2014. Sadly, there is no end in sight. Maine’s Attorney General Janet Mills declared that drug overdose deaths are up 50% in 2016, with the first 6 months of the year experiencing 189 drug overdose deaths alone. What’s worse, the number of overdose-related deaths in 2016 is expected to reach a new record, surpassing those numbers of 2014 and 2015.

“Heroin addiction is devastating our communities,†Maine Governor Paul LePage said in a statement. “For many, it all started with the overprescribing of opioid pain medication.â€
As a state with the largest number of patients per capita on prescription for long-acting opioids, the news that prescribed pain medication is further fueling opioid addiction is unsettling.
This is why Maine has decided to take action.
Maine’s new statue, “An Act to Prevent Opiate Abuse by Strengthening the Controlled Substances Prescription Monitoring Program,†entails a number of rules and regulations designed to reduce the harm of over-prescribing opioids relative to the abuse and misuse of such substances. This bill, signed into law by Governor LePage, mandates a number of changes for doctors and dentists who prescribe controlled substances in Maine.
[Read: The Maine Mandate – Confronting Controlled Substances Head-On]
What changes will be implemented?
Dosing and Duration of Schedule II Medications
First, this law imposes limitations on the medication dosage, as well as the duration of a prescription, that can be prescribed to a patient. According to Gordon Smith, JD, Executive Vice President of Maine Medical Association (MMA), the original bill limited opioid prescriptions to three days for acute pain and fifteen days for chronic pain. However, this legislation will now mandate a limit of seven days for acute pain and thirty days for chronic pain on opioid prescriptions. This law goes in to effect January 1, 2017.
In terms of dosing, prescribers may not prescribe any combination of opioid medication in an aggregate amount of more than 100 Morphine Milligram Equivalents (MMEs) per day to new opioid patients (after July 29, 2016). Existing opioid patients with active prescriptions in excess of 100 MMEs per day are referred to as “Legacy Patients†and prescribers may not prescribe any combination of opioid medication in an aggregate amount of more than 300 MMEs per day from July 29, 2016 to July 1, 2017.
Prescription Monitoring Program
Maine prescribers are required to query the Prescription Monitoring Program (PMP) database prior to prescribing opiates. Although this requirement has been in place since 2005, surveys indicate that only 7-20% of Maine prescribers currently utilize the state’s PMP.
The purpose of checking this central state database is to identify patients who may be doctor shopping and minimize multiple controlled substance prescriptions for one patient. This aligns with the state’s hope of empowering healthcare providers to recognize potential substance abuse and treat patients accordingly.
PMP’s can also be most effective when linked with an e-Prescribing solution. Working together, e-Prescribing eliminates the need for paper prescriptions, thus reducing the risk of altered dispense quantities, stolen prescriptions or prescription pads, and the reselling of such prescriptions before they’re filled as a means of lessening the red flags if a patient is doctor shopping.
[Read: The Link Between PDMP’s and e-Prescribing]
Continuing Education
Via this statute, prescribers must complete three hours of continuing education every two years as a condition of prescribing opioid medications. This specific addiction training is only required if a prescriber wishes to continue prescribing opioids.
Electronic Prescribing
All opioid prescriptions must be sent electronically as of July 1, 2017.
What exceptions are part of this mandate?
The Maine Medical Association (MMA) confirms that exceptions from the law’s provisions may be granted for the following:
- Cancer Patients
- Hospice Care
- End-of-Life Care
- Palliative Care
- Patients on Medication-Assisted Therapy (MAT)
- Patients receiving medication in hospitals and nursing homes
The MMA is currently seeking an exception for burn victims as well.
Due to the supremacy clause of the U.S. Constitution, federal law takes priority over state law, therefore prescribers within the Department of Veterans Affairs (the VA) cannot be regulated by this type of legislation so long as the medication is dispensed at a VA pharmacy. Furthermore, dosage and duration limits would not apply to a prescription written for a veteran by a prescriber outside of the VA system if the prescription were filled in a VA pharmacy.
How does this bill measure up?
With this bill, Maine becomes the third state behind Minnesota and New York to require e-Prescribing and the second to require the electronic sending of a controlled substance after New York imposed a similar mandate in March of 2016. Since the implementation of New York’s mandate, total numbers of opioid analgesics prescribed fell by 78% within the first four months.
Important dates to remember:
|
7/29/2016
|
Prescribers may not prescribe any combination of opioid medication in an aggregate amount of more than 100 Morphine Milligram Equivalents (MMEs) per day to new opioid patients |
|
7/29/2016 – 7/1/2017
|
Prescribers may not prescribe any combination of opioid medication in an aggregate amount of more than 300 MMEs per day to “Legacy Patients†|
|
1/1/2017
|
Duration limitation goes into effect. All opioid prescriptions cannot exceed seven days for acute pain or thirty days for chronic pain. |
| 7/1/2017 |
All opioid prescriptions must be sent electronically |
Lastly, as part of the state’s strategy, Maine has launched Dose of Reality, a website to help educate and inform their citizens of the dangers of painkillers and where to turn for help.
Author: Lindsey W.
Sources:Â Maine Medical Association; Maine.gov; Medscape; WCSH6; Bangor Daily News
About DoseSpot
DoseSpot is a Surescripts certified e-Prescribing platform specifically designed to integrate with electronic health record, electronic dental record, practice management and telehealth software. DoseSpot is certified to e-Prescribe controlled substances and has provided simple, affordable and integratable e-Prescribing solutions to healthcare IT companies since 2009. For more information, please visit www.DoseSpot.com.
Posted: October 27th, 2016 | Author: Shauna | Filed under: Basics, Controlled Substances, In the News, Public Policy, Security, Standards | Tags: Controlled Substances, DEA, DoseSpot, e-Prescribing, e-Prescribing controlled substances, e-Prescribing Integration, e-Prescribing Software, electronic prescribing, Healthcare Software, Opioid Epidemic, Opioids, Patient Engagement, PDMP, PMP, Prescription Drug Monitoring Program, Prescription Monitoring Program, State Mandates, trends, Value Based Care | No Comments »

On par with our last post, the widespread media attention and devastating losses associated with our nation’s current opioid epidemic has sparked certain state legislatures to regulate and improve providers’ prescribing habits for prescription painkillers.
With good intentions in tow, some rulings seem to lack readily available solutions that are proven to curb this crisis. However, they do realize that their recent proposals do not mark the end of this uphill battle, rather multifaceted solutions need to be in place to truly, and successfully, overcome this epidemic.
[Read: Overdose Awareness – The Time to Stand Together is Now]
Here are three states that have recently proposed rulings on how opioids should be prescribed:
Vermont
Coined as a “cutting-edge†approach to overcoming the opioid crisis, Governor Peter Schumlin announced proposed limits on the number of opioid medications that could be prescribed.
Like every other state, Vermont has seen an incredible increase in deaths related to opioid and heroin overdose in recent years and Governor Schumlin is no longer sitting on the sidelines.
Earlier this year, he approached both the FDA and pharmaceutical industry in his State of the State address claiming that OxyContin “lit the match that ignited America’s opiate and heroin addiction crisis,†and that the booming American opiate industry knows no shame, an outcry after the FDA approved OxyContin for children a few months ago.
The proposed ruling states that the severity and duration of pain will determine the specific limit for a prescription of opioids. For example, a minor procedure with moderate pain would be limited to 9-12 opioid pills and the amount would increase based on the procedure performed and the level of pain a patient claims. The ruling would also require providers to discuss risks, provide an education sheet to the patient and receive an informed consent for all first-time opioid prescriptions.
The Green Mountain State’s Governor believes that limiting the number of opioid pills prescribed would be an effective way to reduce addiction, yet some folks believe the ruling would only encourage patients to seek illicit drugs elsewhere if they cannot receive pain medication through their provider.
This does make sense considering many former and current heroin abusers have stated that their addiction started from a prescription and when the pill bottle ran out, they were left seeking these drugs on the streets, which have proven to be very, if not more, dangerous than the prescription.
However, the intent of the Governor’s ruling is to prevent addiction from ever happening in the first place. His ruling is specific to cases of acute pain, therefore changing the over-prescribing habits and learned behavior of utilizing opioids as first-line therapy; habits that ensued in large part due to incentives, the surge of pharmaceutical marketing tactics and claims that painkillers were not addictive.
[Read: How Costly Are Prescription Pain Meds?]
New Jersey
With the rate of drug overdose deaths on the rise by 137% since 2000, New Jersey is another state to recently propose new regulations on how and to whom opioids are prescribed.
New Jersey, much like many other states, believes that prevention is key when fighting this crisis and they couldn’t be more correct. Unfortunately, several barriers often occur when seeking appropriate treatment after a patient becomes addicted, (for example, providers are limited to certain amounts for which they can administer reversal drugs), and therefore why not PREVENT addiction, rather than simply TREAT addiction when at many times, it’s too late?
Senator Raymond Lesniak has introduced a bill that would put restrictions on health insurance coverage for opioid medications, while also requiring prescribers to first consider alternative pain-management treatments, follow federal prescribing guidelines and explain the risk of addiction with such substances to their patients before prescribing. Furthermore, providers will need to complete several steps before receiving approval of an opioid prescription. These steps include providing a patient’s medical history, conducting a physical exam and developing an appropriate medical plan for treating a patient’s pain.
While new rulings in place can certainly shift this epidemic, Angela Valente, the executive director of the Partnership for a Drug-Free New Jersey, said it best:
“Awareness and education is the key factor in preventing the abuse of opiates—everyone must have a role in reversing this epidemic, including lawmakers, parents, coaches, educators, and yes, even doctors and dentists.†– Angela Valente
Dr. Andrew Kolodny, executive director of Physicians Responsible for Opioid Prescribing, further backs Valente’s point while also motioning that the medical community has been prescribing too aggressively.
[Read: The Opioid Epidemic: Are Dentists the Black Sheep?]
Pennsylvania
Unfortunately, Pennsylvania experienced 3,500 deaths last year as a result from drug overdose, one of the highest overdose rates in the nation.
The state has had a Prescription Drug Monitoring Program for quite a few years now, however it wasn’t functional until August 2016, when their new program was officially rolled out. Pennsylvania requires providers to query the state’s prescription drug database the first time they prescribe a controlled substance to a patient or if they have reason to believe that the patient is doctor shopping.
Governor Tom Wolf addressed other initiatives underway including requiring providers to query the database EACH time they prescribe opioids, updating medical school curriculum and continuing education, changes to the process of pain care to lower inappropriate use of opioids, and improved screening, referral and treatment for addiction.
What’s bothersome in Pennsylvania, is the method in which these substances have to be prescribed. The Pennsylvania Controlled Substance Act requires narcotic prescriptions to be handwritten on paper prescription pads, yet every other substance can be electronically prescribed. This allows the risk of written prescriptions being lost, stolen, or sold. Luckily, Senator Richard Alloway intends to introduce this measure before the legislative session’s end.
It’s promising to see how the above states are utilizing their state’s Prescription Drug Monitoring Program, or PDMP. All three require their prescribers to query the affiliated state database, however the parameters in which, or how often, they check varies.
While said efforts are better than no effort at all and states are starting to fully understand the need for multifaceted solutions in order to overcome this epidemic, one key solution is missing. E-Prescribing.
[Read: The Link Between PDMP’s and e-Prescribing]
How does e-Prescribing help combat this epidemic?
- e-Prescribing diminishes the possibilities of duplicate or lost prescriptions since the prescription is sent directly to the patient’s pharmacy
- A patient will no longer have a paper prescription where the dispense quantity can be altered
- Prescribers will have access to a patient’s medication history, therefore they can determine if a patient is “doctor shopping†or has a history of substance abuse
To learn how to incorporate e-Prescribing as a solution to the opioid epidemic, schedule a meeting with DoseSpot today.
Sources:Â NY Times; Boston.com; ABC News; Press of Atlantic City; PennLive
About DoseSpot
DoseSpot is a Surescriptsâ„¢ certified e-Prescribing platform specifically designed to integrate with electronic health record, electronic dental record, practice management and telehealth software. DoseSpot is certified to e-Prescribe controlled substances and has provided simple, affordable and integratable e-Prescribing solutions to healthcare IT companies since 2009. For more information, please visit www.DoseSpot.com.
Posted: October 20th, 2016 | Author: Shauna | Filed under: Controlled Substances, In the News, Standards | Tags: Controlled Substances, DEA, e-Prescribing, e-Prescribing controlled substances, MA PAT, MA PMP, Massachusetts PMP, Massachusetts Prescription Awareness Tool, Massachusetts Prescription Monitoring Program, Massachusetts State Mandate, MassPAT, Opioid Epidemic, Opioids, Patient Engagement, PDMP, PMP, Prescription Drug Monitoring Program, Prescription Monitoring Program, State Mandates, Value Based Care | No Comments »
For the first 6 months of 2016 in Massachusetts, there have been almost 500 confirmed cases of unintentional opioid overdose deaths and an estimated 500 additional cases have not yet been confirmed.
The majority of overdoses found in MA are due to substances such as fentanyl and heroin, but rates of cocaine and benzodiazepines present in opioid deaths have been steady since 2014. Although the rates of heroin and prescription drugs present in opioid deaths have been decreasing due to many efforts that have been implemented across the nation, the rate of fentanyl has been on the rise. This is in large part due to the fact that many opioid addictions start at the hands of a prescriber with a prescription and when the pill bottle runs dry, patients are left seeking other options that produce the same euphoric effect.

With the rapid increase of deaths and devastation by way of the current opioid epidemic plaguing the state, Massachusetts has recently implemented further requirements concerning practitioner’s prescribing protocols. Specifically, with the state’s Prescription Monitoring Program, or PMP.
The PMP serves as a database for all prescription drugs that are dispensed across the state, including those that are highly sought after for non-medical use and represent the highest potential for abuse, better known as Schedule II-V drugs such as narcotics, sedatives, and stimulants.
When properly used, the PMP aids in the identification and prevention of drug misuse, diversion, and potential doctor shopping by providing a patient’s medication history of the past 12 months. It is meant to be utilized as a key clinical decision-making tool that allows providers to receive a big picture view of the patient they are treating in real time.
As a solution to this widespread epidemic, Massachusetts has introduced new legislation and requirements when utilizing the MassPAT (Massachusetts Prescription Awareness Tool).
Effective October 15, 2016, practitioners must abide by the following:
- A registered individual practitioner must utilize the prescription monitoring program each time the practitioner issues a prescription to a patient EACH time for a narcotic drug in Schedule II or III.
- A registered individual practitioner must utilize the prescription monitoring program prior to prescribing to a patient for the first time:
- A benzodiazepine; OR
- Any controlled substance in Scheduled IV or V which the department has designated in guidance as a drug that is commonly abused and may lead to dependence. At this time, there are no drugs that have received this designation.
Prior to the aforementioned requirements, legislation ruled that practitioners, among other factors, need only check the state PMP when prescribing a controlled substance to a patient for the first time, while it is now required for a practitioner to check the system EVERY time when prescribing Schedule II or III drugs.
An example of just how serious Massachusetts is about this crisis, and also believed to be the first agreement of its kind, CVS recently paid almost $800k to the state because pharmacists were not checking prescriptions or the database thoroughly. In exchange, CVS agreed to provide its pharmacists access to the PMP website, train its pharmacists to register for and use the PMP as appropriate, and has further agreed to implement policies that would require pharmacists to consult the PMP before dispensing certain opioids in MA.
Massachusetts and CVS, among many other organizations, recognize the importance of the state’s PMP as a tool to detect and prevent the abuse and misuse of controlled substances. The PMP is not meant to be another government-controlled, green monster hanging on a practitioner’s back at all times; it is meant to serve as a safety extension for practitioners, but most importantly for their patients.
PMP’s can also be most effective when linked with an e-Prescribing solution. Working together, e-Prescribing eliminates the need for paper prescriptions, thus reducing the risk of altered dispense quantities, stolen prescriptions or prescription pads, and the reselling of such prescriptions before they’re filled as a means of lessening the red flags if a patient is doctor shopping.
About DoseSpot
DoseSpot is a Surescriptsâ„¢ certified e-Prescribing platform specifically designed to integrate with electronic health record, electronic dental record, practice management and telehealth software. DoseSpot is certified to e-Prescribe controlled substances and has provided simple, affordable and integratable e-Prescribing solutions to healthcare IT companies since 2009. For more information, please visit www.DoseSpot.com.
Posted: August 31st, 2016 | Author: Shauna | Filed under: Basics, Controlled Substances, In the News, Public Policy | Tags: CBS News, CNN, Controlled Substances, e-Prescribing, e-Prescribing of Controlled Substances, EPCS, International Overdose Awareness Day, Opioid Epidemic, Opioid Prescriptions, Opioids, Overdose Awareness Day, PDMPs, Shatterproof, State Mandates, Time Magazine | No Comments »
International Overdose Awareness Day
To some, this day may not mean much, but to others, it is a day to commemorate and remember loved ones that we lost as a result of overdose. Unfortunately, these fatal occurrences are in large part due to a horrible, stigmatized and chronic illness: addiction.
While there has been widespread media attention for how addiction “should†be categorized as outlined in the latest New York Times article, addiction, specifically with opioids, is still viewed as a moral failing, a flaw, even. The associated stigma often deters patients from receiving proper rehabilitation treatment and even if they do seek treatment, the government currently limits the number of patients a single provider may treat with drugs such as buprenorphine or methadone, which are both proven to reduce cravings and save lives. This leads to many patients relapsing.
Physicians, internists, and dentists are collectively responsible for providing 81.6% of opioid prescriptions in the United States and because of this, they have a very unique role in mitigating the impact of this opioid epidemic. Opioid addiction often starts at the hands of healthcare professionals simply trying to do their job, prescribing pain medications to relieve their patients of painful woes, especially during post-operative recovery.
While many prescriptions are meant for initial, short-term treatment, some doctors and dentists authorize refills time and time again because they want to help patients whom claim that they are still in pain. However, when the pill bottle and refills run out, these patients are left high and dry; looking for alternatives to create that euphoric escape they’ve become so accustomed to. This could mean an endless search of several different doctors to prescribe more substances (also known as doctor shopping), purchasing pills on the black market, or worse, turning to heroin as a cheaper and more readily available alternative.
As the Surgeon General, Dr. Vivek Murthy, reiterates in his recent letter to all of America’s doctors, many prescribers don’t realize how dangerous the drugs can be, or even how addictive they are because many were incorrectly taught that opioids are not addictive when prescribed for legitimate pain. Dr. Murthy further points out that overdose deaths from opioids have quadrupled since 1999 and pain medication prescriptions have risen to the point that there’s enough for every American adult to have their own bottle of pills. It’s a fair statement that the majority of clinicians do not enter the healthcare industry with intent to harm their patients, yet it’s also fair to say that lack of proper education has further fueled these prescribing patterns.
So, who’s to blame here? Is it the prescribers? The pharmaceutical companies’ aggressive marketing tactics in the 1990’s? Learned behaviors? The demands and expectations from patients?
The truth of the matter is: no one is to blame. Blaming only diverts the necessary explication of collectively coming together as a nation to address this epidemic. The imperative solution is education.
Dr. Murthy also addresses in his letter that now is the time for clinicians to properly educate themselves on how to treat pain safely and effectively and screen patients for opioid use disorder and provide them with helpful resources and evidence-based treatment options. Furthermore, to shape how the rest of the country sees addiction, clinicians should shamelessly speak about it and start treating it as a chronic illness.
As a part of this ongoing education initiative, DoseSpot will be hosting a webinar in regards to the opioid epidemic that will include helpful tips and resources to stay ahead of this crisis. Stay tuned for more details.
Sources: Time; CNN; Time; Aetna; Surgeon General Letter; Shatterproof; CBS News
About DoseSpot:
DoseSpot is a Surescripts certified e-Prescribing platform specifically designed to integrate with electronic health record, electronic dental record, practice management and telehealth software. DoseSpot is certified to e-Prescribe controlled substances and has provided simple, affordable and integratable e-Prescribing solutions to healthcare IT companies since 2009. For more information, please visit http://www.DoseSpot.com.
 Follow
Follow