Posted: March 23rd, 2017 | Author: Shauna | Filed under: Controlled Substances, Dental | Tags: Controlled Substances, DEA, Dental, Dental e-Prescribing, dental practice management, Dental Support Organization, DSO, e-Prescribing, e-Prescribing controlled substances, electronic prescribing, EPCS, Great Expressions Dental Centers, Opioid Epidemic, Opioids, Patient Engagement, PDMP, Prescription Drug Monitoring Program | No Comments »

To continue our round table blog series, we shed light from the technical side of dentistry’s role in the opioid epidemic. This time, we sat down with Jason Wolan, Director of EHR Implementation at Great Expressions Dental Centers.
How does your organization view the opioid epidemic as well as your dentists’ role in this crisis?
Great Expressions Dental Centers recognizes an opioid epidemic in this country driven largely by what has historically been a very lax approach to responsible prescribing. Today a lack of commitment by major stakeholders to take hard stances on better regulating the manufacturing and supply of these drugs continues to fuel the fire. In many cases, exploration of alternative pain management therapies and more rigid prescribing protocols that mitigate excess supply and drive more frequent doctor-patient interaction for those on long-term pain management therapies would likely result in major strides to not only reduce excess supply, but reduce unnecessary consumption as well. As a leading DSO and supplier of these medications, it is our job in the dental industry to lead by example and set progressive prescribing protocols that focus on responsible pain management therapies reinforced by firm controls and processes that deter abuse.
Are you having internal conversations about how your organization can curb the use of opioids or dispense trends?
Internally, our transition to an electronic prescribing platform has really been the catalyst for all of this primarily allowing us to gain insight into the prescribing habits of our providers. Prior to prescribing electronically, we relied heavily on spotty computerized provider order entry (CPOE) and “good faith” prescribing based on paper prescriptions being written with little or no audit trail. Today, we are phasing out paper prescribing with an ultimate goal of reporting on prescribing habits, particularly as they relate to opioid prescribing, allowing us better insight into drug-volume and drug-frequency combinations that may raise red flags.
How do you think e-Prescribing assists in efforts to curb opioid prescribing habits?
First and foremost, e-Prescribing, as is the case with most transitions to electronic mediums, will allow for better organizational oversight which will likely cause an industry shift as providers begin to recognize the results of increased transparency. Access to this aggregated data will create an unprecedented level of ad-hoc and scheduled reporting of prescribing habits with the ability to begin to profile behaviors and automatically intervene as necessary. In the past, while prescribing could be tracked, much of the data was burdensome and time consuming to compile, but as electronic prescribing platforms and the industry standards have become so available, the ease with which most organizations can monitor and proactively engage providers today should be a major driving force in deterring abusive prescribing. Reinforcing the latter will come with a societal transformation of less tolerance for prescriber supported prescription drug abuse and the increased media coverage, both at the state and federal level, prosecuting the offending prescribers.
Do you have access to data that you currently, or plan to, utilize in regards to proving how your practices are focused on responsibly prescribing these substances?
Great Expressions Dental Centers is currently generating weekly reports of prescribing focused on drug-volume/drug-frequency combinations. While the organization has not completely transitioned to electronic prescribing, we have significantly reduced access to paper prescribing and expect to see the true value of electronic prescribing when we are able to profile our organizational prescribing practices in its entirety.
Are there any policies in place, or may be in the future, regarding how many pills should be dispensed per controlled substance?
As a DSO, our clinical operations, policies, and procedures, and guidelines are all set by our Chief Clinical Officer. A consistent patient experience defined by responsible care coordination for all Great Expressions Dental Center’s patients is the cornerstone of the brand we have established. A large part of that includes driving responsible practicing techniques and ensuring that our patients’ interests are front and foremost, this of course includes responsible prescribing to mitigate the risks associated with opioid prescribing and has existed prior to our engagement with electronic prescribing. In the future, we hope to leverage the platform further in this regard.
To listen to the full round table, download your copy here.
Some responses have been slightly edited for clarity and length.
About DoseSpot
DoseSpot is a Surescripts certified e-Prescribing platform specifically designed to integrate with electronic health record, electronic dental record, practice management and telehealth software. DoseSpot is certified to e-Prescribe controlled substances and has provided simple, affordable and integratable e-Prescribing solutions to healthcare IT companies since 2009. For more information, please visit www.DoseSpot.com.
Posted: March 22nd, 2017 | Author: Shauna | Filed under: Controlled Substances, Dental | Tags: Controlled Substances, DEA, Dental, Dental Associates, Dental e-Prescribing, dental practice management, Dental Support Organization, DSO, e-Prescribing, e-Prescribing controlled substances, electronic prescribing, EPCS, Opioid Epidemic, Opioids, Patient Engagement, PDMP, Prescription Drug Monitoring Program | No Comments »

As the opioid epidemic continues to grow across the nation, DoseSpot recently sat down with Key Opinion Leaders from Dental Support Organizations (DSOs) to discuss how their organization is implementing best practices to decrease opioid overdose deaths and increase patient safety, as well as their viewpoint on what dentistry’s role is during this crisis.
For part I of our blog series, our focus is on the clinical element of dentistry’s role in the opioid epidemic with Dr. John Zweig, Chief Dental Officer of Dental Associates.
How does your organization view the opioid epidemic as well as your dentists’ role in this crisis?
Dental Associates is keenly aware of the problem with opioids and we take a very deliberate role in managing patients’ pain appropriately with the minimum required medication. Educating patients and matching pain relief management with the present dental problem is very important.
Do you provide your dentists education, training, or resources regarding controlled substances?
Continually, Dental Associates has educated its providers on appropriate pain control measures and the use of controlled drugs. The challenge remains with patients whom insist on strong medications and working with them to minimize the prescriptions and the type of drugs used. More patient education is required, and our use of patient prescription histories is becoming more widely used to discover how to explain the minimum amount of medication used.
Within your dental practices, how do you communicate the important relationship between dentists and controlled substances?
Within our provider education, orientation and our monitoring of prescriptions, we continue to provide feedback to minimize prescriptions for controlled drugs both in type and quantity of medication provided.
How do you think e-Prescribing assists in efforts to curb opioid prescribing habits?
It actually reduces fraud; it ensures that we are writing the prescriptions the way we want them to be and that they get to the right people. Electronic prescriptions allows us to monitor this because potentially we may have a provider who is unknowingly or unwittingly giving out large amounts of drugs and we can have a conversation with them, potentially educate them, or make them aware of the situation. This isn’t about a “gotcha game,” it’s about educating providers on best practices.
How do you handle/communicate with patients that may have a substance abuse issue?
Well, many times, first, we use the Wisconsin prescription drug monitoring program (PDMP). That has been in existence and the state has been encouraging us to use it. When using it, we find that many of the patients we’re concerned about are in pain management programs and so we refer them back to their pain managers to resolve their pain needs, so we’re not making it too complicated. For those not in a pain management program, we communicate the facts on their known prescriptions and advise them that we may be unable to prescribe more. We discover with that information, the push-back is minimal.
Anything else you think would be relevant in addressing dentistry’s role in curbing this epidemic?
The issue is a big problem, but I still think it requires education for patients and also the providers, because people have the expectation to reduce demand for pain medication. We need to educate the doctors on best practices with medications that are not controlled substances. We need to monitor and educate everyone.
Stay tuned for Part II: DSOs’ technical insight into dentistry’s role in the opioid epidemic.
To listen to the full round table, download your copy here.
Some responses have been slightly edited for clarity and length.
About DoseSpot
DoseSpot is a Surescripts certified e-Prescribing platform specifically designed to integrate with electronic health record, electronic dental record, practice management and telehealth software. DoseSpot is certified to e-Prescribe controlled substances and has provided simple, affordable and integratable e-Prescribing solutions to healthcare IT companies since 2009. For more information, please visit www.DoseSpot.com.
Posted: February 8th, 2017 | Author: DoseSpot | Filed under: Basics, Controlled Substances, Public Policy | Tags: Addiction, Addiction Treatment, American Medical Association, CDC, Controlled Substances, DEA, Drug Diversion, e-Prescribing controlled substances, e-Prescribing State Law, EPCS, Maine State Mandate, Mandatory e-Prescribing, Mandatory Electronic Prescribing, PDMP, PDMP State Law, PDMPs, PMP, PMPs, Prescription Drug Abuse, Prescription Drug Diversion, Prescription Drug Monitoring Program, Prescription Drug Monitoring Programs, Prescription Monitoring Program, Prescription Monitoring Programs, State Law, State Mandate | No Comments »

Prescription Drug Monitoring Programs (PDMPs) are state-run electronic databases that are used to track the prescribing and dispensing of controlled prescription drugs with the intent of helping to detect suspected abuse or diversion. These electronic databases provide important information regarding a patient’s controlled substance history that can be accessed by authorized individuals or agencies including law enforcement, medical examiners, addiction treatment programs, public and private payers, pharmacies, healthcare providers, and more.
All states except Missouri, the District of Columbia, and Guam have enacted PDMP legislation that mandate healthcare providers to record, consult and monitor prescribing data. Since the widespread implementation of PDMPs and corresponding legislations, there have been stories and statistics that seem to indicate success, however, there has also been feedback that indicates some major troubles with these databases and their use.
With PDMPs being utilized all over the country, should we expect a major turn-around in the prescription opioid crisis that is sweeping the nation? Are these databases in fact doing the job that they are intended to do? Or, are there major issues that are preventing their success? Let’s explore together.
The Benefits of PDMPs
PDMPs are considered to be the most promising state-level interventions to improve opioid prescribing, inform clinical practice, and protect patients at risk. They are intended to not only medically benefit patient care, but also to serve as a tool for law enforcement and other agencies concerned with opioid-related threats to the public health. This is because the information entered in to a PDMP can help prescribers and pharmacists identify patients at high-risk who would benefit from early interventions.
Further evaluations of PDMPs have demonstrated changes in prescribing behaviors, the use of multiple providers by patients, and decreased substance abuse treatment admissions. From a public health standpoint, PDMPs can be used by state health departments to better understand the current opioid addiction epidemic to better create new intervention methods.
As an example, in 2010, Florida established a PDMP and prevented health care providers from dispensing prescription opioid pain relievers directly from their office. That same year, there was a 50% decrease in oxycodone overdose deaths in the state. This change is thought to represent the first documented, substantial decline in drug overdose mortality in any state during the previous ten years.
Likewise, in 2012, prescribers in New York and Tennessee were required to check the state’s PDMP before prescribing opioids and the following year, New York saw a 75% drop in patients “doctor shopping†and Tennessee saw a 36% drop.
The Unfortunate Reality of PDMPs
Although PDMPs have significant potential to improve public health and patient outcomes, they do have the following shortcomings:
1. Under-Utilization
The inconsistent use, or under-utilization, of PDMPs is considered to be the biggest issue plaguing the database, as a PDMP is most useful when queried before prescribing and most maximized where usage is state mandated. A recent survey found that with physicians prescribing in a state without a PDMP mandate, only 22% were aware of their state’s PDMP, and only 53% had actually used it. These facts clearly indicate that state legislation is a critical success factor for the effectiveness of PDMPs to save patient lives.
2. Lack of Accessibility
Another issue with PDMPs is the ease of use and access, or lack thereof. States vary widely in which user categories are permitted to request and receive prescription history reports and under what conditions. Research suggests that usage may improve if states were to allow providers to appoint non-prescribing staff members to access the database on their behalf.
Furthermore, not all PDMPs share information across state lines. This can lead to important information being missed and can allow at-risk patients to receive more prescriptions for controlled substances than intended. However, more states are realizing the importance of sharing data across state lines and have recently become a part of PMP InterConnect.
3. Varying Times of Information Entry
Another matter of concern with PDMPs is varying times of information entry. When a controlled substance is dispensed to a patient, the prescription and patient information is entered by the pharmacy to the state PDMP. However, this information is entered at varying intervals – hourly, daily, or even monthly. If there is a long interval between dispense and submission times into the state PDMP, users will not have the most up-to-date information on a patient’s most recent prescriptions, thereby eliminating the maximum benefit of a PDMP. Currently, Oklahoma is the only state that collects data in real time, whereas, most states allow up to a week or longer for data submission.
4. Patient Adoption
Many prescribers attribute their worry about a patient’s reaction when checking the PDMP as a major disadvantage. In a recent survey, providers reported a variety of issues that arose when they reviewed the PDMP:
- 88% of patients reacted with anger or denial when questioned
- 73% of clinicians said that those angered patients sometimes did not return
- 22% of clinicians reported that the confronted patients had never asked for help with drug addiction or dependence problems
These clinicians also indicated that the unveiling of this information was not only upsetting to patients, and damaging to practitioner-patient relationships, but was also found to be inaccurate at times.
Additional concerns include added costs of more frequent office visits if prescribers become more cautious about writing prescriptions with refills, feelings of embarrassment when questioned about substance abuse, and patients turning to the illicit drug market if they are refused a controlled substance prescription.
Although the American Medical Association and American Society of Addiction Medicine stress the need to treat PDMP data just as well, if not better, than any other medical record, patients are becoming more vocal in their discomfort with PDMPs, claiming they make them feel that a medical consultation is no longer private.
5. Reluctant Prescribers
Like their patients, prescribers also show growing concern that they will be judged based on PDMP data. While most prescribers are assumed to support interventions to prevent fraudulent prescribing, high profile criminal prosecutions of prescribing large amounts of opioids can make prescribers reluctant to prescribe controlled substances in general for fear of legal retribution, also known as the “chilling effectâ€.
There is also greater perceived legal risk for prescribing or dispensing too much pain medication than for prescribing or dispensing too little pain medication. Because many practicing physicians have little if any formal training that would enable them to identify drug diversion, there is fear that PDMPs may wrongfully suspect and categorize some conscientious and caring physicians as fraudulent prescribers when they are actually prescribing in good faith, but lack training.
What Does This All Mean?
In this era of information technology, PDMPs are likely here to stay. While there are the aforementioned pitfalls of PDMPs, it is important to remember that there are still benefits to PDMPs in the public health sector, law enforcement, and of course, healthcare systems. What may be most helpful is to realize what changes could be made to make the PDMP process an ideal one.
From the standpoint of many prescribers, an ideal PDMP would:
- Alert its users to signs of illegal drug use
- Be easy to access
- Provide real time updates
- Be mandatory
- Have interstates accessibility
Perhaps over time if these changes were to be made, we would see more consistent use of PDMPs, especially as a tool to help overcome the opioid epidemic. A clear standard of practice against which providers’ care would be judged could also further advance the utilization of PDMPs in each state. Lastly, adequate training on addiction and pain management, along with a careful review of who should access a PDMP, could also attribute to better utilization and help accelerate the acceptance of each states’ prescription drug monitoring programs.
Author: Lindsey W.
Sources: Centers for Disease Control and Prevention; Lynn Webster MD; PDMP Assist;Â Wolters Kluwer; Shatterproof; National Center for Biotechnology Information
About DoseSpot
DoseSpot is a Surescripts certified e-Prescribing platform specifically designed to integrate with electronic health record, electronic dental record, practice management and telehealth software. DoseSpot is certified to e-Prescribe controlled substances and has provided simple, affordable and integratable e-Prescribing solutions to healthcare IT companies since 2009. For more information, please visit www.DoseSpot.com.
Posted: January 23rd, 2017 | Author: DoseSpot | Filed under: Basics, Controlled Substances | Tags: CMS, Controlled Substances, DEA, e-Prescribing, e-Prescribing controlled substances, e-Prescribing Integration, EPCS, health IT, healthcare IT, Maine State Mandate, meaningful use, Opioid Epidemic, State Mandates, surescripts | No Comments »

Navigating the waters of e-Prescribing can seem like a very daunting task considering the various state and federal regulations. To assist you in understanding, let’s review the information relative to e-Prescribing of Controlled Substances (EPCS) in all 50 states and how your state is measuring up.
Until recently, one-half of all U.S. States prohibited e-Prescribing of controlled substances. The thought was that paper prescriptions were safer and more secure. On September 15, 2015, however, Vermont became the last state to allow electronic prescribing of controlled substances, or Schedule II-V medications, making this process legal in all 50 U.S. states.
“We certainly believe that because of the enhanced security associated with e-Prescribing of controlled substances, the opportunity for abuse, misuse, and fraudulent activity is going to be dramatically reduced,” said Ken Whittemore, BSPharm, MBA, Senior Vice President of Professional and Regulatory Affairs at Surescriptsâ„¢, a nationwide health information network.
With this process now legal in all 50 states, and the safer option at that, it may be surprising to find that as of the most recent data available, only 7% of prescribers are sending controlled substances on the Surescripts network.
So, why the discrepancy? Are pharmacies not accepting electronic prescriptions? Are prescribers not able, or willing, to send these prescriptions electronically? Is this process too difficult? Why is this process used in some states so heavily, but so infrequently in others?
Pharmacies are ready!
In 2010, the DEA published a final ruling giving not only practitioners the option to write controlled substances electronically, but also for pharmacies to receive, dispense, and archive electronic prescriptions.
“It became incumbent upon a number of stakeholder groups in the pharmacy industry to tackle the issue and bring states into alignment with the DEA’s rule,” Ken Whittemore, BSPharm, MBA told Pharmacy Today.
Many pharmacy stakeholder groups, including APhA, the National Alliance of State Pharmacy Associations (NASPA), the National Association of Chain Drug Stores, and Surescripts, worked together over a 5-year period to rework some state laws, a process that can take a long time. Between 2010 and 2015, the pharmacy end of the spectrum worked hard on adoption and enablement, while prescriber enablement trailed. Using data from Surescripts, a study published in the January 2015 American Journal of Managed Care found that pharmacies with technology in place to accept e-Prescriptions for controlled substances increased from 13% in 2012 to 30% in 2013. By contrast, only 1% of all prescribers were capable of e-Prescribing controlled substances in 2013.
However, between 2012 and 2013, the number of e-Prescriptions for controlled substances grew dramatically from 1,535 to 52,423. Talk about a rapid jump!
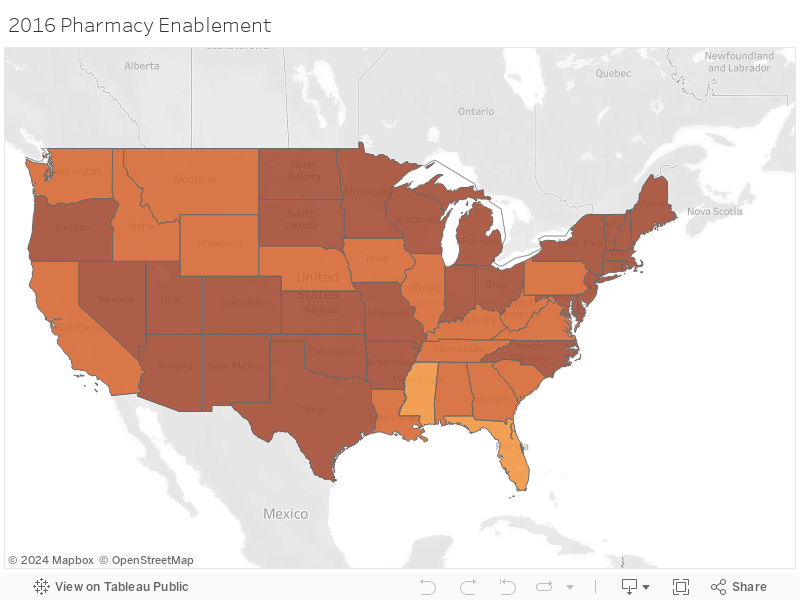
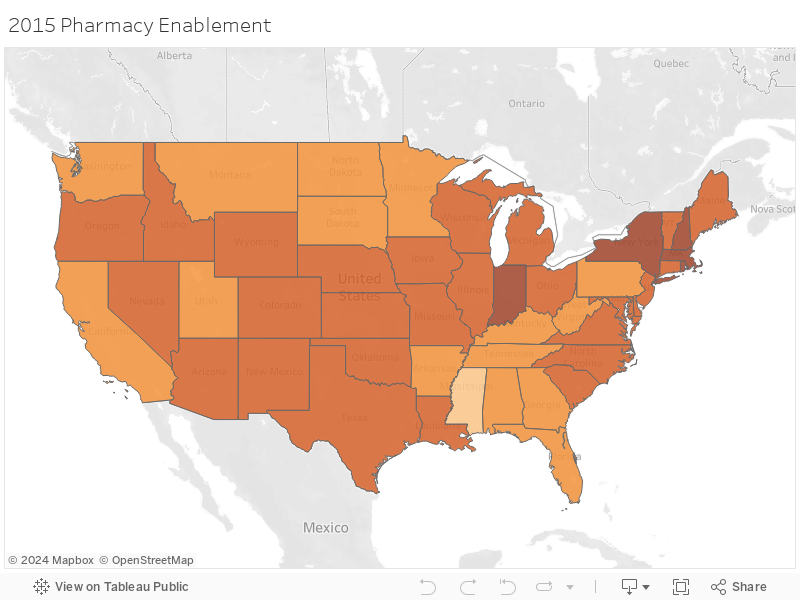
According to the 2015Â Surescripts National Progress Report, an average of 81% of pharmacies were enabled for EPCS in 2015. States including Hawaii and Mississippi were at the bottom of this list with less than 70% of pharmacies enabled, while states in the Northeast such as Massachusetts, New York, New Hampshire, and Rhode Island led this list with over 90% of pharmacies enabled for EPCS.
As of December 1, 2016, these numbers have only risen, with both Hawaii and Mississippi now having over 75% of pharmacies enabled. New York and Maine lead the race on that front with 96.8% and 95.2% of pharmacies enabled currently. This is in large part due to the state mandates put into place in 2016 and 2017, respectfully.
How about the prescribers?
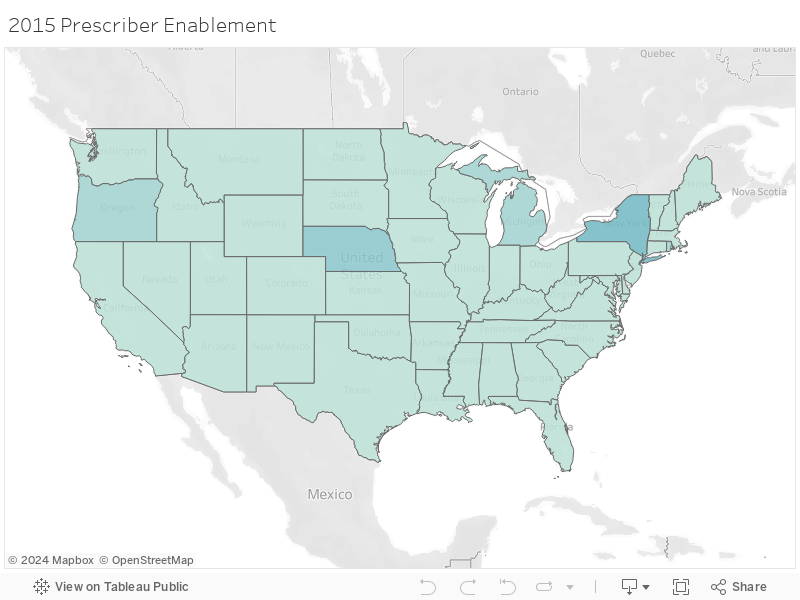
With so many pharmacies enabled for EPCS, and legislature allowing this process in all 50 states, it may be surprising to know that an average of 3.39% of prescribers were enabled to e-Prescribe controlled substances according to the 2015 Surescripts National Progress Report.
Lengthy and time-consuming software auditing and prescriber identity proofing processes are likely factors that have stalled prescriber adoption of EPCS, but for pharmacists, the initial setup is much easier. In addition, there have not been enough incentive for prescribers to adopt EPCS.
e-Prescribing was a requirement under the federal Meaningful Use Electronic Health Record (EHR) program, which incentivizes the use of EHRs through financial payments. However, e-Prescribing of controlled substances was specifically exempted from Meaningful Use Stages 1, 2, and 3. For these reasons, it isn’t surprising that in 2015 the state with the highest number of prescribers enabled was New York, as that was one of the only states with an e-Prescribing state mandate in effect at that time.
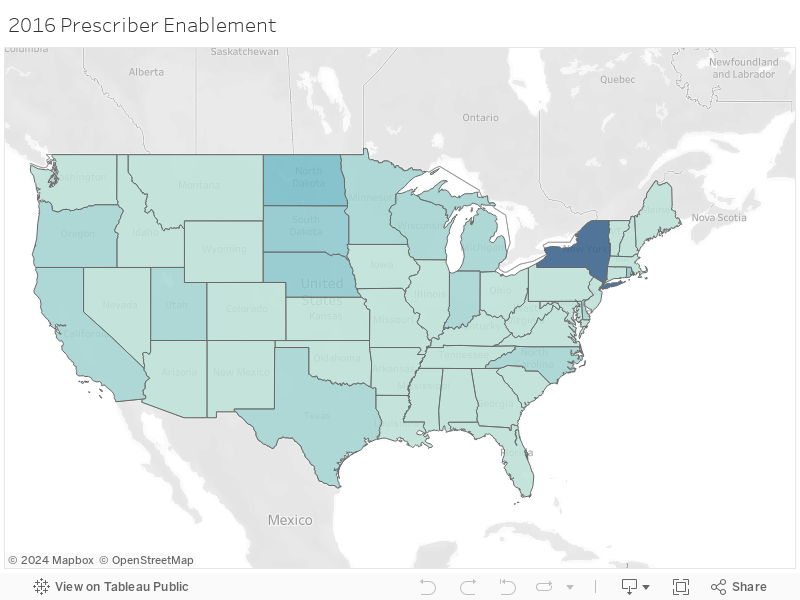
In 2015, New York had 26.6% of their prescribers enabled for EPCS, with Nebraska not far behind at 15%. Fast forward to December 1, 2016 and prescriber enablement has grown tremendously in some states, but remain dismally low in others. New York now has 71.5% of prescribers enabled, with no other state having even one-third of their prescribers enabled for EPCS. In fact, the average percentage for EPCS enabled prescribers remains even as of December 1, 2016, at only 8.4% despite all of the benefits of EPCS.
Why are these numbers so varied?
Electronic prescribing of controlled substances (EPCS) reduces fraud and keeps patients from getting multiple prescriptions for the same drug, so why are some states seeing major buy-in while other states are lagging? Much of this is impacted by states that have legislation in place to either require or reinforce the use of e-Prescribing, as outlined below.
Minnesota
Minnesota was the first state to implement an e-Prescribing mandate in 2008 in order to improve quality outcomes and efficiency in health care. The state mandate required prescribers, pharmacists, pharmacies, and pharmacy benefit managers (PBMs) to be up and running with e-Prescribing by January 1, 2011, however, only 13% of prescribers are actually enabled for EPCS as of late. Could this be because legislation doesn’t enforce its own law or penalize prescribers for not adhering to this legislature? Marty LaVenture, director of the Minnesota Office of Health IT and e-Health, seems to agree and notes, “policy levers could be used to encourage full adoption and use of e-Prescribing capabilities.”
New York
As you may already know, New York was the first state to require e-Prescribing of all prescriptions, both controlled and non-controlled, and the first to implement penalties for failing to adhere to this ruling. Penalties include, but are not limited to, loss of license, civil penalties, and/or criminal charges. With the highest rate of prescriber EPCS enablement, it’s evident that New York prescribers are taking this quite seriously.
Maine
Maine is the next state to implement an e-Prescribing regulation as of July 1, 2017 where all opioids prescriptions must be sent electronically. With only 0.6% of prescribers enabled for EPCS in the state according to the Surescripts report, and up to 2.9% as of the beginning of December 2016, it’s clear that Maine has a long way to go for all prescribers to be ready to follow this regulation.
In Summary
Although it’s legal in all 50 states, and there are many reasons EPCS is safer than on paper or another method, there is still a great discrepancy between EPCS enabled pharmacies and EPCS enabled prescribers due in part to the strict requirements put in place on the prescribers. While the statistics referenced here show that provider adoption of EPCS is still low in comparison to the pharmacy adoption we have seen, it’s important to remember that the e-Prescribing of non-controlled substances also took years to reach the level we now see today. It seems the only tried and true way for these numbers to rise quickly and meet the numbers we currently see for pharmacy enablement is to implement regulations and penalties for not adhering to this requirement as outlined in the above state mandates. All eyes are now on Maine to see how their journey goes.
Check out the maps below to see how your state measures up!
Author: Lindsey W.
Sources: American Pharmacists Association; USA Today; Surescripts 2015 National Progress Report; Surescripts EPCS; Minnesota Department of Health; Maine Medical Association; e-Prescribing Blog; CMS
About DoseSpot
DoseSpot is a Surescripts certified e-Prescribing platform specifically designed to integrate with electronic health record, electronic dental record, practice management, and telehealth software. DoseSpot is certified to e-Prescribe controlled substances and has provided simple, affordable and integratable e-Prescribing to more than 150 health care software companies since 2009. For more information, please visit www.DoseSpot.com.
Posted: November 28th, 2016 | Author: DoseSpot | Filed under: Controlled Substances, In the News, Public Policy | Tags: Controlled Substances, DEA, Dental e-Prescribing, e-Prescribing controlled substances, e-Prescribing Integration, e-Prescribing Maine Mandate, EPCS, Healthcare Software, Maine Controlled Substance Act, Maine Controlled Substance Prescription Requirements, Maine Dose of Reality, Maine e-Prescribing Law, Maine e-Prescribing Legislation, Maine e-Prescribing Mandate, Maine e-Prescribing of Controlled Substances, Maine EPCS, Maine Opioid Law, Maine State Mandate, Mandatory e-Prescribing, Mandatory Electronic Prescribing, Opioid Epidemic, Opioids, Prescription Monitoring Program, State Mandates | No Comments »
Maine is well known for its rocky coastline, iconic lighthouses, sandy beaches, and lobster shacks. However, past the classic scenery is where you’ll find the state dealing with a crisis that others across the United States are also experiencing: the opioid epidemic.
In 2015, Maine suffered an astounding 272 drug overdose deaths, following 208 deaths of the same cause in 2014. Sadly, there is no end in sight. Maine’s Attorney General Janet Mills declared that drug overdose deaths are up 50% in 2016, with the first 6 months of the year experiencing 189 drug overdose deaths alone. What’s worse, the number of overdose-related deaths in 2016 is expected to reach a new record, surpassing those numbers of 2014 and 2015.

“Heroin addiction is devastating our communities,†Maine Governor Paul LePage said in a statement. “For many, it all started with the overprescribing of opioid pain medication.â€
As a state with the largest number of patients per capita on prescription for long-acting opioids, the news that prescribed pain medication is further fueling opioid addiction is unsettling.
This is why Maine has decided to take action.
Maine’s new statue, “An Act to Prevent Opiate Abuse by Strengthening the Controlled Substances Prescription Monitoring Program,†entails a number of rules and regulations designed to reduce the harm of over-prescribing opioids relative to the abuse and misuse of such substances. This bill, signed into law by Governor LePage, mandates a number of changes for doctors and dentists who prescribe controlled substances in Maine.
[Read: The Maine Mandate – Confronting Controlled Substances Head-On]
What changes will be implemented?
Dosing and Duration of Schedule II Medications
First, this law imposes limitations on the medication dosage, as well as the duration of a prescription, that can be prescribed to a patient. According to Gordon Smith, JD, Executive Vice President of Maine Medical Association (MMA), the original bill limited opioid prescriptions to three days for acute pain and fifteen days for chronic pain. However, this legislation will now mandate a limit of seven days for acute pain and thirty days for chronic pain on opioid prescriptions. This law goes in to effect January 1, 2017.
In terms of dosing, prescribers may not prescribe any combination of opioid medication in an aggregate amount of more than 100 Morphine Milligram Equivalents (MMEs) per day to new opioid patients (after July 29, 2016). Existing opioid patients with active prescriptions in excess of 100 MMEs per day are referred to as “Legacy Patients†and prescribers may not prescribe any combination of opioid medication in an aggregate amount of more than 300 MMEs per day from July 29, 2016 to July 1, 2017.
Prescription Monitoring Program
Maine prescribers are required to query the Prescription Monitoring Program (PMP) database prior to prescribing opiates. Although this requirement has been in place since 2005, surveys indicate that only 7-20% of Maine prescribers currently utilize the state’s PMP.
The purpose of checking this central state database is to identify patients who may be doctor shopping and minimize multiple controlled substance prescriptions for one patient. This aligns with the state’s hope of empowering healthcare providers to recognize potential substance abuse and treat patients accordingly.
PMP’s can also be most effective when linked with an e-Prescribing solution. Working together, e-Prescribing eliminates the need for paper prescriptions, thus reducing the risk of altered dispense quantities, stolen prescriptions or prescription pads, and the reselling of such prescriptions before they’re filled as a means of lessening the red flags if a patient is doctor shopping.
[Read: The Link Between PDMP’s and e-Prescribing]
Continuing Education
Via this statute, prescribers must complete three hours of continuing education every two years as a condition of prescribing opioid medications. This specific addiction training is only required if a prescriber wishes to continue prescribing opioids.
Electronic Prescribing
All opioid prescriptions must be sent electronically as of July 1, 2017.
What exceptions are part of this mandate?
The Maine Medical Association (MMA) confirms that exceptions from the law’s provisions may be granted for the following:
- Cancer Patients
- Hospice Care
- End-of-Life Care
- Palliative Care
- Patients on Medication-Assisted Therapy (MAT)
- Patients receiving medication in hospitals and nursing homes
The MMA is currently seeking an exception for burn victims as well.
Due to the supremacy clause of the U.S. Constitution, federal law takes priority over state law, therefore prescribers within the Department of Veterans Affairs (the VA) cannot be regulated by this type of legislation so long as the medication is dispensed at a VA pharmacy. Furthermore, dosage and duration limits would not apply to a prescription written for a veteran by a prescriber outside of the VA system if the prescription were filled in a VA pharmacy.
How does this bill measure up?
With this bill, Maine becomes the third state behind Minnesota and New York to require e-Prescribing and the second to require the electronic sending of a controlled substance after New York imposed a similar mandate in March of 2016. Since the implementation of New York’s mandate, total numbers of opioid analgesics prescribed fell by 78% within the first four months.
Important dates to remember:
|
7/29/2016
|
Prescribers may not prescribe any combination of opioid medication in an aggregate amount of more than 100 Morphine Milligram Equivalents (MMEs) per day to new opioid patients |
|
7/29/2016 – 7/1/2017
|
Prescribers may not prescribe any combination of opioid medication in an aggregate amount of more than 300 MMEs per day to “Legacy Patients†|
|
1/1/2017
|
Duration limitation goes into effect. All opioid prescriptions cannot exceed seven days for acute pain or thirty days for chronic pain. |
| 7/1/2017 |
All opioid prescriptions must be sent electronically |
Lastly, as part of the state’s strategy, Maine has launched Dose of Reality, a website to help educate and inform their citizens of the dangers of painkillers and where to turn for help.
Author: Lindsey W.
Sources:Â Maine Medical Association; Maine.gov; Medscape; WCSH6; Bangor Daily News
About DoseSpot
DoseSpot is a Surescripts certified e-Prescribing platform specifically designed to integrate with electronic health record, electronic dental record, practice management and telehealth software. DoseSpot is certified to e-Prescribe controlled substances and has provided simple, affordable and integratable e-Prescribing solutions to healthcare IT companies since 2009. For more information, please visit www.DoseSpot.com.
Posted: November 8th, 2016 | Author: Shauna | Filed under: Basics, Controlled Substances, Dental | Tags: Controlled Substances, DEA, Dental, Dental e-Prescribing, dental practice management, e-Prescribing controlled substances, e-Prescribing Integration, e-Prescribing Software, electronic prescribing, EPCS, health IT, healthcare IT, Healthcare Software, healthIT, Opioid Epidemic, Opioids, Patient Engagement, technology, trends, Value Based Care | No Comments »

Unfortunately, the opioid epidemic that is currently grappling the United States isn’t exactly news. Headlines appear on a daily basis in regards to this addiction, the overdoses and fatalities, as well as the healthcare community’s contribution to this crisis, both the good and the bad.
We’ve seen Congress, the Surgeon General, and many other organizations make extreme efforts to combat this crisis, yet despite the widespread media attention, many healthcare professionals still don’t realize how dangerous the drugs can be or how addictive they are.
DoseSpot recently conducted a live webinar in an effort to educate and discuss the critical role that dentists in particular play in mitigating the current opioid epidemic that is upon us and during that time, the following crucial points were made:
The blame game needs to stop
Blaming others only diverts the necessary action of collectively coming together as a nation, regardless of one’s associated industry. Healthcare, Law Enforcement, Politics – there needs to be a strong, unified foundation for which we can assemble and fight this battle together.
Break the habit: prescribing patterns of pain medication
Dentists serve a unique role in overcoming this epidemic due to the nature of their work and the procedures they perform, specifically wisdom teeth extraction. It’s a fair statement that the majority do not enter the healthcare industry with ill intent of harming their patients, yet it’s also fair to say that lack of proper education and prior pharmaceutical marketing tactics have fueled poor prescribing patterns. In order to change one’s behavior, programmed thoughts and approaches must be reevaluated.
Opioid addiction does not discriminate
This addiction can affect anyone regardless of one’s socioeconomic status or in some cases, a person’s relationship to their dentist. What DoseSpot coins as “The Insider Threat,” we reveal how certain folks pose a potential risk relative to obtaining controlled substances, both knowingly and secretively. Stories of addiction that are shared during our recent webinar further prove that opioids do not discriminate.
Solutions are available
The truth of the matter is, there is not one single solution that can work independently. It needs to be a collective effort and innovation is critical to success. There needs to be multifaceted solutions to tackle this complex problem ranging from increasing specialty training and education to proper treatment technology, data, and analytics.
To learn more on dentistry’s role in the opioid epidemic, watch the full webinar here.
Presenters:
Greg Waldstreicher, CEO, DoseSpot
Dr. John Zweig, Chief Dental Officer, Dental Associates
Donald Whamond, Chief Technology Officer, Dental Associates
Jason Wolan, Director of EHR Implementation, Great Expressions Dental Centers
Daniel Smelter, Director of Business Analysis, Benevis, Inc.
About DoseSpot
DoseSpot is a Surescripts certified e-Prescribing platform specifically designed to integrate with electronic health record, electronic dental record, practice management and telehealth software. DoseSpot is certified to e-Prescribe controlled substances and has provided simple, affordable and integratable e-Prescribing solutions to healthcare IT companies since 2009. For more information, please visit www.DoseSpot.com.
Posted: October 27th, 2016 | Author: Shauna | Filed under: Basics, Controlled Substances, In the News, Public Policy, Security, Standards | Tags: Controlled Substances, DEA, DoseSpot, e-Prescribing, e-Prescribing controlled substances, e-Prescribing Integration, e-Prescribing Software, electronic prescribing, Healthcare Software, Opioid Epidemic, Opioids, Patient Engagement, PDMP, PMP, Prescription Drug Monitoring Program, Prescription Monitoring Program, State Mandates, trends, Value Based Care | No Comments »

On par with our last post, the widespread media attention and devastating losses associated with our nation’s current opioid epidemic has sparked certain state legislatures to regulate and improve providers’ prescribing habits for prescription painkillers.
With good intentions in tow, some rulings seem to lack readily available solutions that are proven to curb this crisis. However, they do realize that their recent proposals do not mark the end of this uphill battle, rather multifaceted solutions need to be in place to truly, and successfully, overcome this epidemic.
[Read: Overdose Awareness – The Time to Stand Together is Now]
Here are three states that have recently proposed rulings on how opioids should be prescribed:
Vermont
Coined as a “cutting-edge†approach to overcoming the opioid crisis, Governor Peter Schumlin announced proposed limits on the number of opioid medications that could be prescribed.
Like every other state, Vermont has seen an incredible increase in deaths related to opioid and heroin overdose in recent years and Governor Schumlin is no longer sitting on the sidelines.
Earlier this year, he approached both the FDA and pharmaceutical industry in his State of the State address claiming that OxyContin “lit the match that ignited America’s opiate and heroin addiction crisis,†and that the booming American opiate industry knows no shame, an outcry after the FDA approved OxyContin for children a few months ago.
The proposed ruling states that the severity and duration of pain will determine the specific limit for a prescription of opioids. For example, a minor procedure with moderate pain would be limited to 9-12 opioid pills and the amount would increase based on the procedure performed and the level of pain a patient claims. The ruling would also require providers to discuss risks, provide an education sheet to the patient and receive an informed consent for all first-time opioid prescriptions.
The Green Mountain State’s Governor believes that limiting the number of opioid pills prescribed would be an effective way to reduce addiction, yet some folks believe the ruling would only encourage patients to seek illicit drugs elsewhere if they cannot receive pain medication through their provider.
This does make sense considering many former and current heroin abusers have stated that their addiction started from a prescription and when the pill bottle ran out, they were left seeking these drugs on the streets, which have proven to be very, if not more, dangerous than the prescription.
However, the intent of the Governor’s ruling is to prevent addiction from ever happening in the first place. His ruling is specific to cases of acute pain, therefore changing the over-prescribing habits and learned behavior of utilizing opioids as first-line therapy; habits that ensued in large part due to incentives, the surge of pharmaceutical marketing tactics and claims that painkillers were not addictive.
[Read: How Costly Are Prescription Pain Meds?]
New Jersey
With the rate of drug overdose deaths on the rise by 137% since 2000, New Jersey is another state to recently propose new regulations on how and to whom opioids are prescribed.
New Jersey, much like many other states, believes that prevention is key when fighting this crisis and they couldn’t be more correct. Unfortunately, several barriers often occur when seeking appropriate treatment after a patient becomes addicted, (for example, providers are limited to certain amounts for which they can administer reversal drugs), and therefore why not PREVENT addiction, rather than simply TREAT addiction when at many times, it’s too late?
Senator Raymond Lesniak has introduced a bill that would put restrictions on health insurance coverage for opioid medications, while also requiring prescribers to first consider alternative pain-management treatments, follow federal prescribing guidelines and explain the risk of addiction with such substances to their patients before prescribing. Furthermore, providers will need to complete several steps before receiving approval of an opioid prescription. These steps include providing a patient’s medical history, conducting a physical exam and developing an appropriate medical plan for treating a patient’s pain.
While new rulings in place can certainly shift this epidemic, Angela Valente, the executive director of the Partnership for a Drug-Free New Jersey, said it best:
“Awareness and education is the key factor in preventing the abuse of opiates—everyone must have a role in reversing this epidemic, including lawmakers, parents, coaches, educators, and yes, even doctors and dentists.†– Angela Valente
Dr. Andrew Kolodny, executive director of Physicians Responsible for Opioid Prescribing, further backs Valente’s point while also motioning that the medical community has been prescribing too aggressively.
[Read: The Opioid Epidemic: Are Dentists the Black Sheep?]
Pennsylvania
Unfortunately, Pennsylvania experienced 3,500 deaths last year as a result from drug overdose, one of the highest overdose rates in the nation.
The state has had a Prescription Drug Monitoring Program for quite a few years now, however it wasn’t functional until August 2016, when their new program was officially rolled out. Pennsylvania requires providers to query the state’s prescription drug database the first time they prescribe a controlled substance to a patient or if they have reason to believe that the patient is doctor shopping.
Governor Tom Wolf addressed other initiatives underway including requiring providers to query the database EACH time they prescribe opioids, updating medical school curriculum and continuing education, changes to the process of pain care to lower inappropriate use of opioids, and improved screening, referral and treatment for addiction.
What’s bothersome in Pennsylvania, is the method in which these substances have to be prescribed. The Pennsylvania Controlled Substance Act requires narcotic prescriptions to be handwritten on paper prescription pads, yet every other substance can be electronically prescribed. This allows the risk of written prescriptions being lost, stolen, or sold. Luckily, Senator Richard Alloway intends to introduce this measure before the legislative session’s end.
It’s promising to see how the above states are utilizing their state’s Prescription Drug Monitoring Program, or PDMP. All three require their prescribers to query the affiliated state database, however the parameters in which, or how often, they check varies.
While said efforts are better than no effort at all and states are starting to fully understand the need for multifaceted solutions in order to overcome this epidemic, one key solution is missing. E-Prescribing.
[Read: The Link Between PDMP’s and e-Prescribing]
How does e-Prescribing help combat this epidemic?
- e-Prescribing diminishes the possibilities of duplicate or lost prescriptions since the prescription is sent directly to the patient’s pharmacy
- A patient will no longer have a paper prescription where the dispense quantity can be altered
- Prescribers will have access to a patient’s medication history, therefore they can determine if a patient is “doctor shopping†or has a history of substance abuse
To learn how to incorporate e-Prescribing as a solution to the opioid epidemic, schedule a meeting with DoseSpot today.
Sources:Â NY Times; Boston.com; ABC News; Press of Atlantic City; PennLive
About DoseSpot
DoseSpot is a Surescriptsâ„¢ certified e-Prescribing platform specifically designed to integrate with electronic health record, electronic dental record, practice management and telehealth software. DoseSpot is certified to e-Prescribe controlled substances and has provided simple, affordable and integratable e-Prescribing solutions to healthcare IT companies since 2009. For more information, please visit www.DoseSpot.com.
Posted: October 20th, 2016 | Author: Shauna | Filed under: Controlled Substances, In the News, Standards | Tags: Controlled Substances, DEA, e-Prescribing, e-Prescribing controlled substances, MA PAT, MA PMP, Massachusetts PMP, Massachusetts Prescription Awareness Tool, Massachusetts Prescription Monitoring Program, Massachusetts State Mandate, MassPAT, Opioid Epidemic, Opioids, Patient Engagement, PDMP, PMP, Prescription Drug Monitoring Program, Prescription Monitoring Program, State Mandates, Value Based Care | No Comments »
For the first 6 months of 2016 in Massachusetts, there have been almost 500 confirmed cases of unintentional opioid overdose deaths and an estimated 500 additional cases have not yet been confirmed.
The majority of overdoses found in MA are due to substances such as fentanyl and heroin, but rates of cocaine and benzodiazepines present in opioid deaths have been steady since 2014. Although the rates of heroin and prescription drugs present in opioid deaths have been decreasing due to many efforts that have been implemented across the nation, the rate of fentanyl has been on the rise. This is in large part due to the fact that many opioid addictions start at the hands of a prescriber with a prescription and when the pill bottle runs dry, patients are left seeking other options that produce the same euphoric effect.

With the rapid increase of deaths and devastation by way of the current opioid epidemic plaguing the state, Massachusetts has recently implemented further requirements concerning practitioner’s prescribing protocols. Specifically, with the state’s Prescription Monitoring Program, or PMP.
The PMP serves as a database for all prescription drugs that are dispensed across the state, including those that are highly sought after for non-medical use and represent the highest potential for abuse, better known as Schedule II-V drugs such as narcotics, sedatives, and stimulants.
When properly used, the PMP aids in the identification and prevention of drug misuse, diversion, and potential doctor shopping by providing a patient’s medication history of the past 12 months. It is meant to be utilized as a key clinical decision-making tool that allows providers to receive a big picture view of the patient they are treating in real time.
As a solution to this widespread epidemic, Massachusetts has introduced new legislation and requirements when utilizing the MassPAT (Massachusetts Prescription Awareness Tool).
Effective October 15, 2016, practitioners must abide by the following:
- A registered individual practitioner must utilize the prescription monitoring program each time the practitioner issues a prescription to a patient EACH time for a narcotic drug in Schedule II or III.
- A registered individual practitioner must utilize the prescription monitoring program prior to prescribing to a patient for the first time:
- A benzodiazepine; OR
- Any controlled substance in Scheduled IV or V which the department has designated in guidance as a drug that is commonly abused and may lead to dependence. At this time, there are no drugs that have received this designation.
Prior to the aforementioned requirements, legislation ruled that practitioners, among other factors, need only check the state PMP when prescribing a controlled substance to a patient for the first time, while it is now required for a practitioner to check the system EVERY time when prescribing Schedule II or III drugs.
An example of just how serious Massachusetts is about this crisis, and also believed to be the first agreement of its kind, CVS recently paid almost $800k to the state because pharmacists were not checking prescriptions or the database thoroughly. In exchange, CVS agreed to provide its pharmacists access to the PMP website, train its pharmacists to register for and use the PMP as appropriate, and has further agreed to implement policies that would require pharmacists to consult the PMP before dispensing certain opioids in MA.
Massachusetts and CVS, among many other organizations, recognize the importance of the state’s PMP as a tool to detect and prevent the abuse and misuse of controlled substances. The PMP is not meant to be another government-controlled, green monster hanging on a practitioner’s back at all times; it is meant to serve as a safety extension for practitioners, but most importantly for their patients.
PMP’s can also be most effective when linked with an e-Prescribing solution. Working together, e-Prescribing eliminates the need for paper prescriptions, thus reducing the risk of altered dispense quantities, stolen prescriptions or prescription pads, and the reselling of such prescriptions before they’re filled as a means of lessening the red flags if a patient is doctor shopping.
About DoseSpot
DoseSpot is a Surescriptsâ„¢ certified e-Prescribing platform specifically designed to integrate with electronic health record, electronic dental record, practice management and telehealth software. DoseSpot is certified to e-Prescribe controlled substances and has provided simple, affordable and integratable e-Prescribing solutions to healthcare IT companies since 2009. For more information, please visit www.DoseSpot.com.
Posted: October 6th, 2016 | Author: Shauna | Filed under: Controlled Substances, Digital Health, Telehealth | Tags: behavioral health, Care Coordination, Controlled Substances, DEA, Dental e-Prescribing, digital health, DoseSpot, e-Prescribing, e-Prescribing controlled substances, e-Prescribing Integration, e-Prescribing Software, EHR, EHR software, EPCS, Geriatric Care, Geriatrics, health IT, healthcare IT, Healthcare Software, healthIT, meaningful use, medication adherence, Opioid Epidemic, Opioids, Patient Engagement, technology, telehealth, telemedicine, trends, Value Based Care | No Comments »

It’s no surprise that technology should be considered a key player as we shift to value-based care. With smartphones, tablets and computers, health information is readily available for patients with a simple click of a button. Why should a consultation with a healthcare professional be any different?
Telehealth greatly increases the scope of the healthcare industry and is bound to open huge opportunities in increasing the quality of healthcare. The ultimate goal here, is to prevent hospital readmissions through better management of individuals with chronic conditions, while also reducing associated costs. By enabling remote patient monitoring and remote access to clinicians, market growth is inevitable as awareness and implementation of standards for reimbursement and adoptions of these care models expands.
While several reports claim that “technology gets in the way of the patient experience,†patients are in fact the ones demanding such access to care. This increase in patient demand for telehealth services has prompted many companies and healthcare organizations to think outside of the box and reevaluate the patient-centric model, while questioning what that care model really means to a patient.
Well, it’s simple. Patients want a customized, cost-effective and convenient healthcare experience to which telehealth can provide.
A recent report states that the global telehealth market was valued at $14.3 Billion in 2014 and is estimated to reach $36.3 Billion by 2020, growing at a CAGR of 14.30% from 2014 to 2020.
With these numbers in tow, we predict the most growth in three different segments:
Behavioral Health and Addiction
As mentioned in a previous post, telehealth has the ability to bridge the gaps in care of behavioral health patients and providers. Not only does it provide a convenient, more comfortable and less expensive medical consultation, but it broadens accessibility to patients whom may not have many options when seeking a behavioral health provider, especially in rural areas. Unfortunately, the lack of psychiatrists and addiction specialists across the nation, as well as the stigma often involved, are contributing to the mental health and addiction issues and creating barriers to appropriate care.
Patients will see their primary care physician and may not receive the exact treatment plan that they need; after all, primary care physicians do not specialize in behavioral health or addiction and often, these illnesses require a lot of time and patience to which the physician may not be able to accommodate. Telehealth will be able to connect patients in need with specialists regardless of their location who know how to treat these specific health issues.
This effective care model will not only lessen the hit on the nation’s bottom line as more and more individuals grapple with suicide, addiction, and other mental health issues, but also revolutionize the way people view the stigma involved and encourage patients to seek help as they are able to receive treatment from the comfort of their own home.
Geriatric Care
Geriatric patients stand to benefit tremendously as a digital health consumer. As mobility can be especially difficult for these patients, the ability to see a physician remotely removes one of the largest barriers to care. Furthermore, transporting patients of this age may potentially do more harm than good.
With telemedicine, providers can more quickly spot at-risk patients and provide interventions to avoid an otherwise unnecessary hospital admission. Similarly, nursing homes can partner with health systems to provide bedside care for their residents at a fraction of the price of an onsite physician.
These infrastructure synergies provide connectivity with electronic health records (EHRs) and create clear communication among hospitals, senior care facilities, referring physicians and patient families. They also provide the link to population based management databases and other health care analytic functions to measure value.
Surgery
Many surgical departments find telehealth to be a more convenient and cost-effective way for pre- and post- operative instructions for procedures of all magnitudes including wisdom teeth extraction, colonoscopies, stent placement and more.
With in-person visits and paper instructions, patients may misinterpret or even forget important information relative to their surgery. This includes what medications to stop taking and how to physically prepare for surgery, while providing a clear, direct line of answers for any questions a patient may have. With instructions digitally delivered prior to surgery, telehealth reduces patient no shows and saves valuable scheduled operating room time.
For post-op patients, providers can check the patient visually, ensuring that patients are following their treatment plans and making adjustments as needed. Through this continuous connection, providers are empowered to deliver the guidance that many patients need as they go through the healing process. These virtual check-ins ensure the patient is on the road to recovery, thus reducing readmission rates all without the patient ever having to leave their home.
Furthermore, telehealth can improve treatment and medication compliance, specifically with controlled substances, i.e. pain medication. Opioid addiction often begins at the hands of a prescriber and with the nation currently facing an opioid epidemic, marrying technology and follow-up appointments when prescribing these types of medications serves as the optimal solution for the safety of all involved.
Technology should no longer be viewed as a barrier to care, but rather embraced in order to improve the healthcare industry, including the improvement of interoperability as well as patient outcomes. Telehealth not only meets the ever increasing demands of patients, but it also assists in preventative care by creating greater access to such care, thus reducing down-the-road costs and burdensome associated with chronic disease. With many chronic diseases being completely preventable, the prevent vs. treat mantra should be sound in every healthcare professional’s mind, while realizing that telehealth is a seamless way of delivering healthcare for all involved.
There may currently be barriers in place regarding reimbursement from payers, but that’s sure to change as more and more payers jump on board for this new delivery model. After all, who’s to say telehealth won’t become the norm and be known as simply….health?
Sources:Â American Well; OpenPR; mHealth Intelligence; Healthcare IT News
About DoseSpot
DoseSpot is a Surescripts certified e-Prescribing platform specifically designed to integrate with electronic health record, electronic dental record, practice management and telehealth software. DoseSpot is certified to e-Prescribe controlled substances and has provided simple, affordable and integratable e-Prescribing solutions to healthcare IT companies since 2009. For more information, please visit www.DoseSpot.com.
Posted: September 13th, 2016 | Author: Shauna | Filed under: Basics, Controlled Substances, Dental | Tags: Controlled Substances, DEA, Dental, Dental e-Prescribing, dental practice management, DoseSpot, e-Prescribing, e-Prescribing controlled substances, e-Prescribing Integration, e-Prescribing Software, EPCS, health IT, healthcare IT, Healthcare Software, healthIT, Opioid Epidemic, Opioids, Oral Health, Patient Engagement | No Comments »

Dental Associates, a leading family group dental practice managing 14 dental clinics and over 100 dentists in Wisconsin, has realized clinical efficiencies and increased patient satisfaction since their launch of DoseSpot’s e-Prescribing of Controlled Substances (EPCS) solution in March of 2015.
Prior to the launch of DoseSpot’s e-Prescribing of Controlled Substances solutions, Dental Associates had deployed e-Prescribing software, but their dentists could only transmit non-controlled prescriptions electronically. As such, dentists wasted time electronically prescribing antibiotics and subsequently printing controlled substance prescriptions. DoseSpot now marries the two and gives Dental Associates’ dentists the ability to streamline care, spend more time with patients and discontinue the use of costly prescription printers and the associated tamper proof prescription paper.
Click here to learn how your company can simplify clinical workflows with e-Prescribing!
“We understand that healthcare technology is shifting and remaining innovative is in Dental Associates’ best interest. Our dentists find DoseSpot to be top-notch and they’re now able to spend more time with their patients rather than running back and forth between the patient’s chair and the prescription printer,†commented Donald Whamond, Chief Technology Officer, Dental Associates. “Printing prescriptions was not only wasting time and money, but also taking valuable time away from the provider-patient relationship.â€
Dental Associates chose DoseSpot as its e-Prescribing partner due to DoseSpot’s unique boutique-style approach to customer service, the ease of e-Prescribing controlled and non-controlled prescriptions, and to enhance the overall security measures surrounding the prescription writing process within Dental Associates’ clinics.
“DoseSpot has made writing prescriptions easier and less time consuming. With the development of my prescription favorites list, it is easy for my staff and I to build a prescription and even change it if need be. Once the prescription is built, it is simple to select and send the prescription to the pharmacy. Life is good with DoseSpot!†said Dr. John Zweig, Chief Dental Officer, Dental Associates.
Register today for our free webinar addressing dentistry and the opioid epidemic on 9/22!
Dental Associates also wanted to stay ahead of the IT curve which in turn has allowed the company to better recruit and attract new dentists.
“Dental Associates prides itself on the patient-centric care model, therefore our patients’ well-being is of utmost priority and DoseSpot simply aligns with our company values,†Whamond added. “We can call any DoseSpot team member at any time and know they will answer right away. That includes Greg Waldstreicher, CEO, DoseSpot.â€
“Like Dental Associates, DoseSpot is committed to offering innovative solutions to the dental market and we put our partners first in everything we do,†said Greg Waldstreicher. “To have the opportunity to deliver a comprehensive, personalized, and integrated platform for Dental Associates is a homerun for both parties.â€
Simplify clinical workflows and improve patient outcomes with DoseSpot e-Prescribing integration for both controlled and non-controlled prescriptions. Schedule your free demo today at www.DoseSpot.com or contact Shauna Leighton, Shauna@DoseSpot.com.
About Dental Associates
Founded in 1973, Dental Associates is Wisconsin’s largest family-owned dental group practice with multiple clinics throughout the state and nearly 800 staff members. Dental Associates provides complete family dental services, both general and specialty dentistry, under one roof, from pediatric dentistry to specialized dental services for older adults with a focus on excellent care that is affordable, accessible and personalized. For additional information please visit www.DentalAssociates.com.
About DoseSpot
DoseSpot is a Surescripts™ certified e-Prescribing platform specifically designed to integrate with electronic health record, electronic dental record, practice management and telehealth software. DoseSpot is certified to e-Prescribe controlled substances and has provided simple, affordable and integratable e-Prescribing solutions to healthcare IT companies since 2009. For more information, please visit www.DoseSpot.com.
 Follow
Follow