e-Prescribing of Controlled Substances – How Does Your State Measure Up?
Posted: January 23rd, 2017 | Author: DoseSpot | Filed under: Basics, Controlled Substances | Tags: CMS, Controlled Substances, DEA, e-Prescribing, e-Prescribing controlled substances, e-Prescribing Integration, EPCS, health IT, healthcare IT, Maine State Mandate, meaningful use, Opioid Epidemic, State Mandates, surescripts | No Comments » Follow
Follow
Navigating the waters of e-Prescribing can seem like a very daunting task considering the various state and federal regulations. To assist you in understanding, let’s review the information relative to e-Prescribing of Controlled Substances (EPCS) in all 50 states and how your state is measuring up.
Until recently, one-half of all U.S. States prohibited e-Prescribing of controlled substances. The thought was that paper prescriptions were safer and more secure. On September 15, 2015, however, Vermont became the last state to allow electronic prescribing of controlled substances, or Schedule II-V medications, making this process legal in all 50 U.S. states.
“We certainly believe that because of the enhanced security associated with e-Prescribing of controlled substances, the opportunity for abuse, misuse, and fraudulent activity is going to be dramatically reduced,” said Ken Whittemore, BSPharm, MBA, Senior Vice President of Professional and Regulatory Affairs at Surescriptsâ„¢, a nationwide health information network.
With this process now legal in all 50 states, and the safer option at that, it may be surprising to find that as of the most recent data available, only 7% of prescribers are sending controlled substances on the Surescripts network.
So, why the discrepancy? Are pharmacies not accepting electronic prescriptions? Are prescribers not able, or willing, to send these prescriptions electronically? Is this process too difficult? Why is this process used in some states so heavily, but so infrequently in others?
Pharmacies are ready!
In 2010, the DEA published a final ruling giving not only practitioners the option to write controlled substances electronically, but also for pharmacies to receive, dispense, and archive electronic prescriptions.
“It became incumbent upon a number of stakeholder groups in the pharmacy industry to tackle the issue and bring states into alignment with the DEA’s rule,” Ken Whittemore, BSPharm, MBA told Pharmacy Today.
Many pharmacy stakeholder groups, including APhA, the National Alliance of State Pharmacy Associations (NASPA), the National Association of Chain Drug Stores, and Surescripts, worked together over a 5-year period to rework some state laws, a process that can take a long time. Between 2010 and 2015, the pharmacy end of the spectrum worked hard on adoption and enablement, while prescriber enablement trailed. Using data from Surescripts, a study published in the January 2015 American Journal of Managed Care found that pharmacies with technology in place to accept e-Prescriptions for controlled substances increased from 13% in 2012 to 30% in 2013. By contrast, only 1% of all prescribers were capable of e-Prescribing controlled substances in 2013.
However, between 2012 and 2013, the number of e-Prescriptions for controlled substances grew dramatically from 1,535 to 52,423. Talk about a rapid jump!
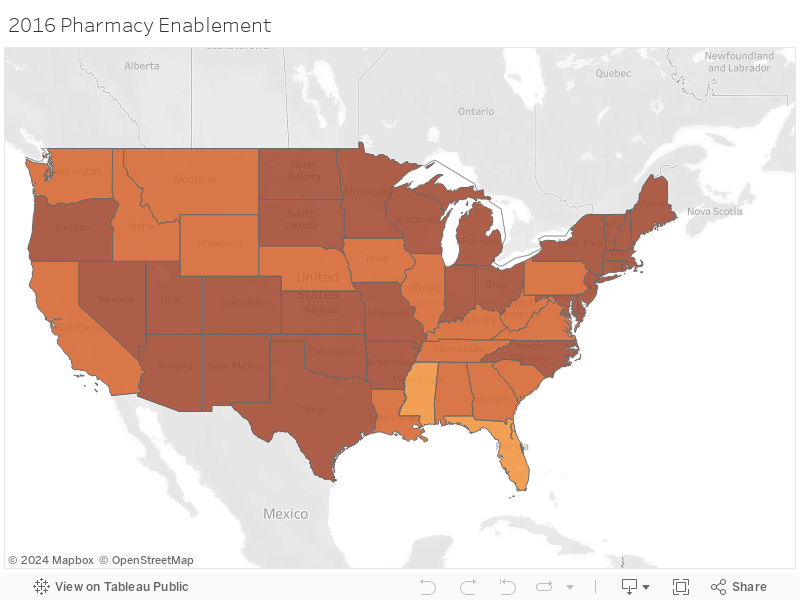
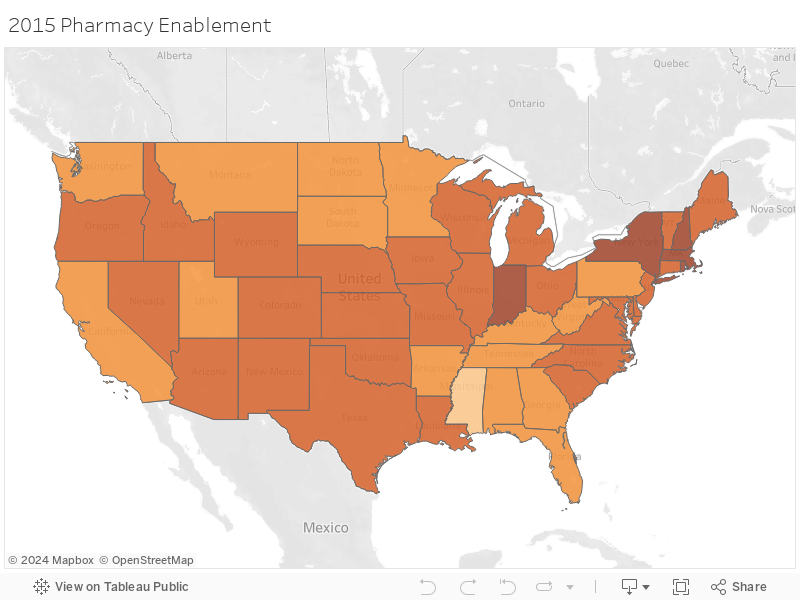
According to the 2015Â Surescripts National Progress Report, an average of 81% of pharmacies were enabled for EPCS in 2015. States including Hawaii and Mississippi were at the bottom of this list with less than 70% of pharmacies enabled, while states in the Northeast such as Massachusetts, New York, New Hampshire, and Rhode Island led this list with over 90% of pharmacies enabled for EPCS.
As of December 1, 2016, these numbers have only risen, with both Hawaii and Mississippi now having over 75% of pharmacies enabled. New York and Maine lead the race on that front with 96.8% and 95.2% of pharmacies enabled currently. This is in large part due to the state mandates put into place in 2016 and 2017, respectfully.
How about the prescribers?
With so many pharmacies enabled for EPCS, and legislature allowing this process in all 50 states, it may be surprising to know that an average of 3.39% of prescribers were enabled to e-Prescribe controlled substances according to the 2015 Surescripts National Progress Report.
Lengthy and time-consuming software auditing and prescriber identity proofing processes are likely factors that have stalled prescriber adoption of EPCS, but for pharmacists, the initial setup is much easier. In addition, there have not been enough incentive for prescribers to adopt EPCS.
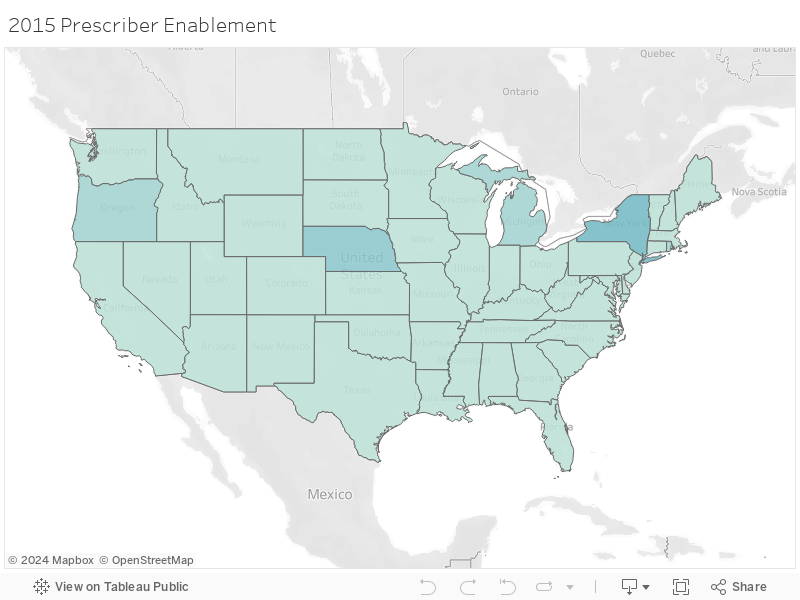
e-Prescribing was a requirement under the federal Meaningful Use Electronic Health Record (EHR) program, which incentivizes the use of EHRs through financial payments. However, e-Prescribing of controlled substances was specifically exempted from Meaningful Use Stages 1, 2, and 3. For these reasons, it isn’t surprising that in 2015 the state with the highest number of prescribers enabled was New York, as that was one of the only states with an e-Prescribing state mandate in effect at that time.
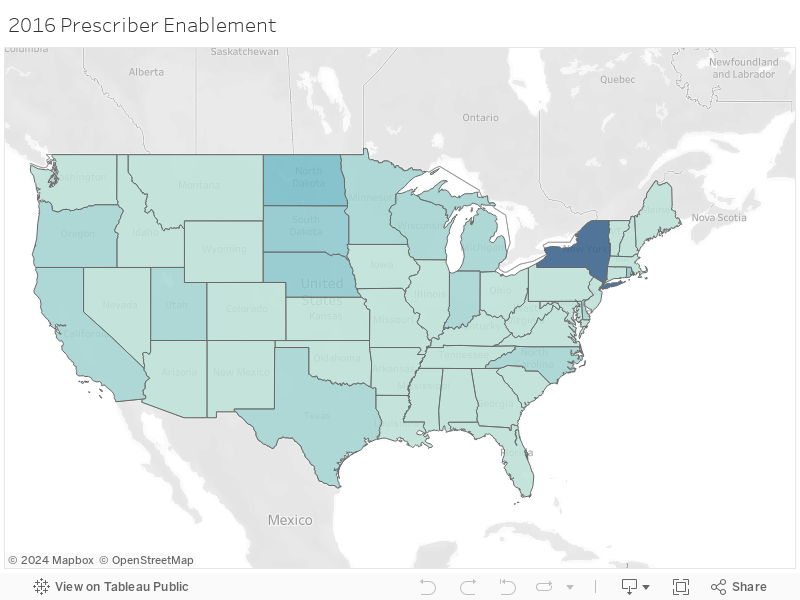
In 2015, New York had 26.6% of their prescribers enabled for EPCS, with Nebraska not far behind at 15%. Fast forward to December 1, 2016 and prescriber enablement has grown tremendously in some states, but remain dismally low in others. New York now has 71.5% of prescribers enabled, with no other state having even one-third of their prescribers enabled for EPCS. In fact, the average percentage for EPCS enabled prescribers remains even as of December 1, 2016, at only 8.4% despite all of the benefits of EPCS.
Why are these numbers so varied?
Electronic prescribing of controlled substances (EPCS) reduces fraud and keeps patients from getting multiple prescriptions for the same drug, so why are some states seeing major buy-in while other states are lagging? Much of this is impacted by states that have legislation in place to either require or reinforce the use of e-Prescribing, as outlined below.
Minnesota
Minnesota was the first state to implement an e-Prescribing mandate in 2008 in order to improve quality outcomes and efficiency in health care. The state mandate required prescribers, pharmacists, pharmacies, and pharmacy benefit managers (PBMs) to be up and running with e-Prescribing by January 1, 2011, however, only 13% of prescribers are actually enabled for EPCS as of late. Could this be because legislation doesn’t enforce its own law or penalize prescribers for not adhering to this legislature? Marty LaVenture, director of the Minnesota Office of Health IT and e-Health, seems to agree and notes, “policy levers could be used to encourage full adoption and use of e-Prescribing capabilities.”
New York
As you may already know, New York was the first state to require e-Prescribing of all prescriptions, both controlled and non-controlled, and the first to implement penalties for failing to adhere to this ruling. Penalties include, but are not limited to, loss of license, civil penalties, and/or criminal charges. With the highest rate of prescriber EPCS enablement, it’s evident that New York prescribers are taking this quite seriously.
Maine
Maine is the next state to implement an e-Prescribing regulation as of July 1, 2017 where all opioids prescriptions must be sent electronically. With only 0.6% of prescribers enabled for EPCS in the state according to the Surescripts report, and up to 2.9% as of the beginning of December 2016, it’s clear that Maine has a long way to go for all prescribers to be ready to follow this regulation.
In Summary
Although it’s legal in all 50 states, and there are many reasons EPCS is safer than on paper or another method, there is still a great discrepancy between EPCS enabled pharmacies and EPCS enabled prescribers due in part to the strict requirements put in place on the prescribers. While the statistics referenced here show that provider adoption of EPCS is still low in comparison to the pharmacy adoption we have seen, it’s important to remember that the e-Prescribing of non-controlled substances also took years to reach the level we now see today. It seems the only tried and true way for these numbers to rise quickly and meet the numbers we currently see for pharmacy enablement is to implement regulations and penalties for not adhering to this requirement as outlined in the above state mandates. All eyes are now on Maine to see how their journey goes.
Check out the maps below to see how your state measures up!
Author: Lindsey W.
Sources: American Pharmacists Association; USA Today; Surescripts 2015 National Progress Report; Surescripts EPCS; Minnesota Department of Health; Maine Medical Association; e-Prescribing Blog; CMS
About DoseSpot
DoseSpot is a Surescripts certified e-Prescribing platform specifically designed to integrate with electronic health record, electronic dental record, practice management, and telehealth software. DoseSpot is certified to e-Prescribe controlled substances and has provided simple, affordable and integratable e-Prescribing to more than 150 health care software companies since 2009. For more information, please visit www.DoseSpot.com.